Impact Summary: This measure supports the Long‑Term Care Hospital (LTCH) Quality Reporting Program goal of measuring and improving the quality of care provided in long‑term care hospitals by assessing LTCH compliance with timely spontaneous breathing trials for patients on mechanical ventilation, a key clinical practice that informs ventilator management, supports care coordination, and improves outcomes for medically complex patients with prolonged hospital stays.
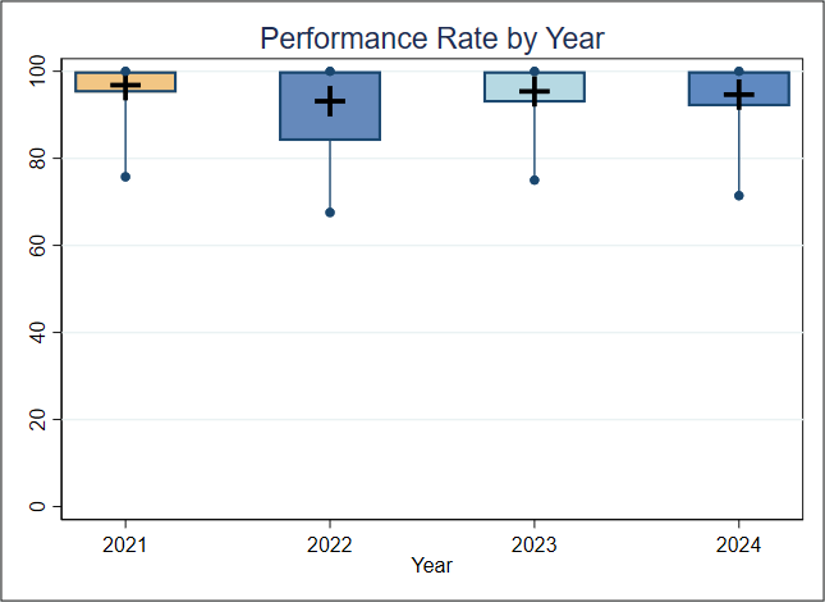
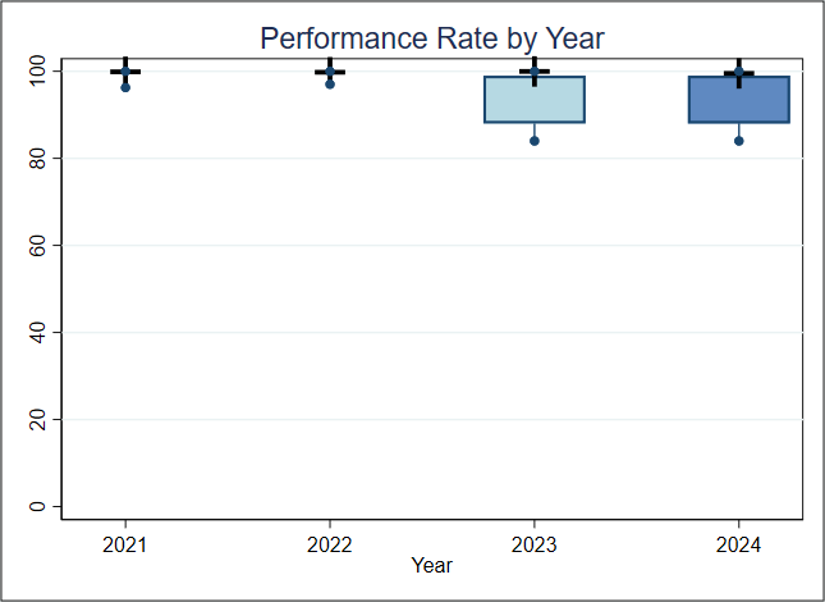
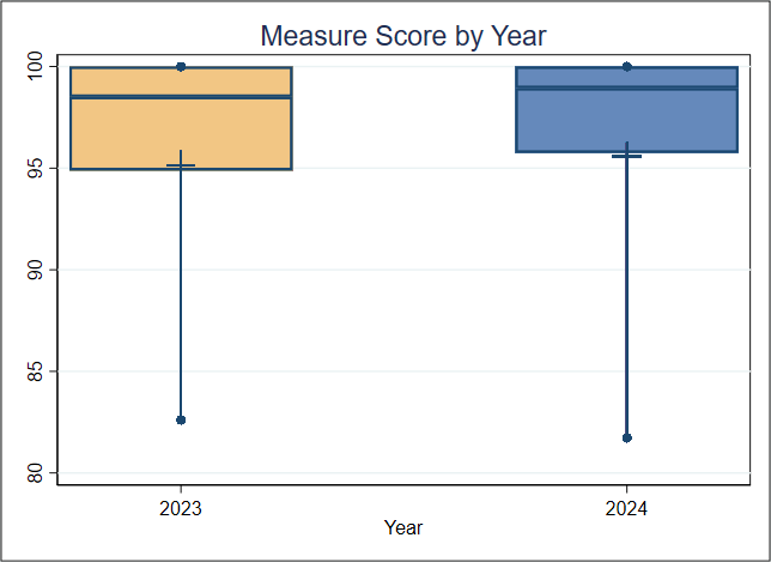
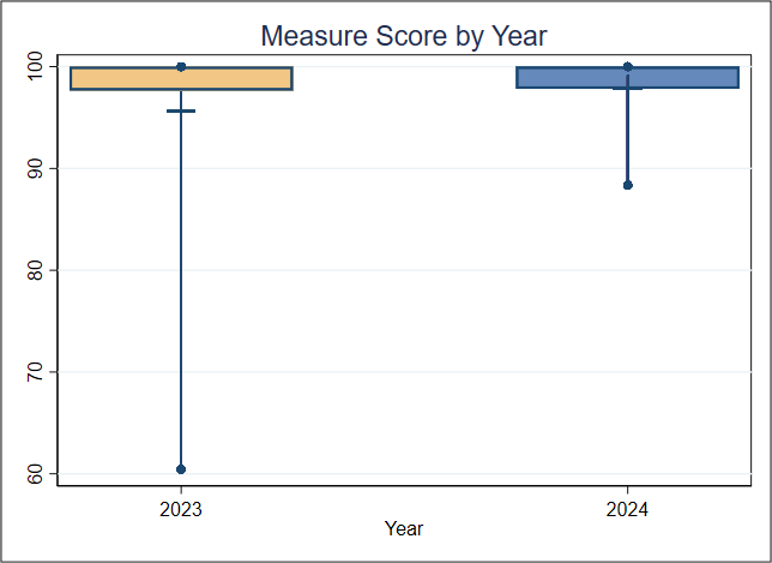
Hospital performance has stayed steady for Component 1 from 2023 to 2024 and increased slightly for Component 2 from 2023 to 2024. For Component 1, the measure identified 23,000 eligible patients assessed for readiness for SBT. Improving performance among lower-scoring hospitals could help ensure about 1,100 patients are assessed for readiness, or about four per entity, potentially leading to better health outcomes. For Component 2, the measure identified 19,100 eligible patients assessed for readiness for SBT. Improving performance among lower-scoring hospitals may help less than two patients per entity; therefore, a benefit may not exceed the entity-level burden of quality data collection.
For this measure, Battelle reviewed the following publicly available datasets available at Long-Term Care Hospital - Provider Data | Provider Data Catalog (cms.gov):
- long-term_care_hospitals_03_2026.zip (which contains data from April 2024-March 2025 and is referred to as year 2024 in this assessment)
- long-term_care_hospitals_03_2025.zip (which contains data from April 2023-March 2024 and is referred to as year 2023 in this assessment)
Battelle analyzed all values for “L_022_02” not marked as “Not Available” from the corresponding Long-term_Care_Hospital-Provider_Data.csv file. We analyzed rates for Component 1 and Component 2 separately.
About Figure 1: Figures 1a and 1b are boxplots that show how scores have changed based on the most recent 2 years of data available. For each year, the boxplot displays a box with lines and dots to help visualize the range and distribution of scores. The dots represent the points where the lowest 5% and highest 5% of scores fall, and the line connecting them shows where 90% of the scores are located. The box itself covers the middle half of the scores, from the 25th to the 75th percentile. Inside the box, a horizontal line marks the median score, which is the middle value, while a “+” sign shows the average score. This type of graph makes overall trends in scores over time as well as the consistency and spread of the results easier to understand.