Percentage of patients assigned female at birth and ages 15-44 who were asked if they wanted to talk about contraception or pregnancy prevention and had their response recorded during the measurement period (which is a calendar year), among patients with a qualifying encounter; to focus on the population of non-postpartum women, the measure excludes those individuals who had a live birth making them eligible for postpartum contraceptive services, and also excludes those who are anatomically infecund or have had female sterilization from the denominator.
Measure Specs
General Information
Supporting patients to prevent pregnancy when they wish to do so has social and health benefits for individuals and their families (1–3). Contraception is a highly effective clinical preventive service that can assist patients in reaching their reproductive health goals (4,5). In order to support patients to achieve their reproductive goals, facilities at which individuals receive care must ensure that their patients’ contraceptive needs are assessed and met. In the care pathway to meeting patients’ contraceptive service needs, healthcare systems and facilities must first identify that the individual desires contraceptive services (see logic model). Building on previous work to optimize contraceptive care and promote positive reproductive health outcomes through the use of performance measures (6–8), the University of California, San Francisco (UCSF) designed the Contraceptive Care Screening eCQM as a process measure to give health care organizations and facilities the ability to monitor and address the provision of screening as a critical part of the contraceptive care pathway that enables those in need of contraceptive services to receive this care.
This measure is aligned with evidence and serves to address a gap in care. Integration of proactive screening for need for pregnancy prevention has been promoted by the Centers for Disease Control and Prevention (CDC) and the American College of Obstetricians and Gynecologists (ACOG) (9,10). However, only 14% of ambulatory visits in the United States include any care related to achieving or preventing pregnancy (11) and only 54% of women report receiving family planning care during the prior 12 months (12). In an analytic sample published this year that included 53,489 patient visits of reproductive age individuals at outpatient care visits, only 8% of visits included family planning services (13). These data indicate that there is a sizeable opportunity to improve integration of contraceptive counseling services into ambulatory care settings. Challenges to providing reproductive health services in primary care have been explored in the research and include uncertainty about patient interest in these conversations and assumptions about patient pregnancy risk and/or desire to discussion pregnancy prevention (14–17). Providers report relying on patients to initiate conversations about contraception (14). This is particularly salient in primary care settings, where many people of reproductive age receive care but where there are many competing priorities that can result in neglect of reproductive health care (18,19).
Implementation of standardized screening for contraceptive care need can address many of these key challenges by overriding provider assumptions about patient preferences and needs and instead asking them directly about their service needs in the care pathway. One study found that after introducing a standardized reproductive health screening tool and training staff on its use, contraceptive counseling increased 24% (20). Implementation of standardized screening can work with other systems-level efforts, including provider training and use of patient decision support tools, to optimize contraceptive care (21). Together training and screening can center reproductive health integration into routine care and can result in increased provision of contraception to those who want the service. A study in a primary care setting found that patients who received contraceptive counseling were more likely to report use of hormonal contraception seven to thirty days post-visit compared to those who did not (22) Moreover, a study of adolescent care delivery found that it took on average three visits for providers to initiate contraceptive counseling, however, once they did, among patients who were not using contraception, 39% left the visit on a method (23).
The Contraceptive Care Screening eCQM complements existing performance measures related to contraceptive care. Currently endorsed measures evaluate provision of contraceptive methods and whether or not counseling was person-centered. The proposed measure adds an additional dimension in the quality care pathway by identifying whether or not people have their needs for contraceptive care evaluated. In addition, this measure is aligned with the endorsed eCQMs of contraceptive use (CBE #3699e and #3682e). Specified for EHR system data, these measures utilize SINC to exclude those from the denominator not interested in contraceptive care in order to focus the measure on the population of patients interested in contraceptive services. Implementing the Contraceptive Care Screening eCQM alone or in combination with other contraceptive care performance measures will result in quality improvement initiatives that help health care organizations better meet clients’ needs by increasing person-centered access to contraception in a wider range of settings, a step towards the goal of reproductive autonomy and well-being for all.
REFERENCES
1. Conde-Agudelo A, Rosas-Bermúdez A, Kafury-Goeta AC. Birth Spacing and Risk of Adverse Perinatal Outcomes: A Meta-analysis. JAMA. 2006 Apr 19;295(15):1809.
2. Conde-Agudelo A, Rosas-Bermúdez A, Kafury-Goeta AC. Effects of birth spacing on maternal health: a systematic review. American Journal of Obstetrics and Gynecology. 2007 Apr;196(4):297–308.
3. Congdon JL, Baer RJ, Arcara J, Feuer SK, Gómez AM, Karasek D, et al. Interpregnancy Interval and Birth Outcomes: A Propensity Matching Study in the California Population. Matern Child Health J. 2022 May;26(5):1115–25.
4. Mansour D, Inki P, Gemzell-Danielsson K. Efficacy of contraceptive methods: A review of the literature. The European Journal of Contraception & Reproductive Health Care. 2010 Feb;15(1):4–16.
5. Trussell J, Aiken ARA, Micks, E, Guthrie K. Efficacy, safety, and personal considerations. In: Contraceptive Technology. 21st ed. )Ayer Company Publishers, Inc.; 2018. p. 95–128.
6. Gavin L, Frederiksen B, Robbins C, Pazol K, Moskosky S. New clinical performance measures for contraceptive care: their importance to healthcare quality. Contraception. 2017 Sep;96(3):149–57.
7. Gavin LE, Ahrens KA, Dehlendorf C, Frederiksen BN, Decker E, Moskosky S. Future directions in performance measures for contraceptive care: a proposed framework. Contraception. 2017 Sep;96(3):138–44.
8. Moniz MH, Gavin LE, Dalton VK. Performance Measures for Contraceptive Care: A New Tool to Enhance Access to Contraception. Obstetrics & Gynecology. 2017 Nov;130(5):1121–5.
9. Johnson K, Posner SF, Biermann J, Cordero JF, Atrash HK, Parker CS, et al. Recommendations to improve preconception health and health care--United States. A report of the CDC/ATSDR Preconception Care Work Group and the Select Panel on Preconception Care. MMWR Recomm Rep. 2006 Apr 21;55(RR-6):1–23.
10. ACOG Committee Opinion No. 762: Prepregnancy Counseling. Obstetrics & Gynecology. 2019 Jan;133(1):e78–89.
11. Bello JK, Rao G, Stulberg DB. Trends in contraceptive and preconception care in United States ambulatory practices. Fam Med. 2015 Apr;47(4):264–71.
12. Borrero S, Schwarz EB, Creinin M, Ibrahim S. The Impact of Race and Ethnicity on Receipt of Family Planning Services in the United States. Journal of Women’s Health. 2009 Jan;18(1):91–6.
13. Schulte A, Biggs MA. Association Between Facility and Clinician Characteristics and Family Planning Services Provided During U.S. Outpatient Care Visits. Women’s Health Issues. 2023 Nov;33(6):573–81.
14. Akers AY, Gold MA, Borrero S, Santucci A, Schwarz EB. Providers’ Perspectives on Challenges to Contraceptive Counseling in Primary Care Settings. Journal of Women’s Health. 2010 Jun;19(6):1163–70.
15. Chuang CH, Hwang SW, McCall‐Hosenfeld JS, Rosenwasser L, Hillemeier MM, Weisman CS. Primary Care Physicians’ Perceptions of Barriers To Preventive Reproductive Health Care In Rural Communities. Perspect Sexual Reproductive. 2012 Jun;44(2):78–83.
16. Zephyrin L, Suennen L, Viswanathan P, Augenstein J, Bachrach D. TRansforming Primary Health Care for Women: Part 1: A Framework for Addressing Gaps and Barriers [Internet]. The Commonwealth Fund; 2020 Jul. Available from: https://www.commonwealthfund.org/sites/default/files/2020-07/Zephyrin_p…
17. Dunlop AL, Jack B, Frey K. National Recommendations for Preconception Care: The Essential Role of the Family Physician. The Journal of the American Board of Family Medicine. 2007 Jan 1;20(1):81–4.
18. Saloner B, Wilk AS, Levin J. Community Health Centers and Access to Care Among Underserved Populations: A Synthesis Review. Med Care Res Rev. 2020 Feb;77(1):3–18.
19. Chen C, Strasser J, Banawa R, Luo Q, Bodas M, Castruccio-Prince C, et al. Who Is Providing Contraception Care in the United States? An Observational Study of the Contraception Workforce. Obstetrical & Gynecological Survey. 2022 Jun;77(6):351–3.
20. Stulberg DB, Dahlquist IH, Disterhoft J, Bello JK, Hunter MS. Increase in Contraceptive Counseling by Primary Care Clinicians After Implementation of One Key Question® at an Urban Community Health Center. Matern Child Health J. 2019 Aug;23(8):996–1002.
21. Borrero S, Callegari L. Integrating Family Planning into Primary Care—a Call to Action. J GEN INTERN MED. 2020 Mar;35(3):625–7.
22. Lee JK, Parisi SM, Akers AY, Borrerro S, Schwarz EB. The Impact of Contraceptive Counseling in Primary Care on Contraceptive Use. J GEN INTERN MED. 2011 Jul;26(7):731–6.
23. Woods JL, Sheeder JL. Missed Opportunities for Discussing Contraception in Adolescent Primary Care. Journal of Pediatric and Adolescent Gynecology. 2020 Dec;33(6):667–72.
The Contraceptive Care Screening eCQM uses Electronic Health Record (EHR) data collected from ambulatory, outpatient clinical encounters and entered into the EHR system. The SINC question and its response options are specified in the LOINC code system (see https://loinc.org/98076-3/) and published online as a value set named “Self Identified Need for Contraception (SINC)” (OID: 2.16.840.1.113762.1.4.1166.115) in the National Library of Medicine (NLM) Value Set Authority Center (VSAC, https://vsac.nlm.nih.gov/ - registration required). This element defines the numerator.
We implemented and tested the Contraceptive Care Screening eCQM in primary care settings through a quality improvement learning collaborative among federally qualified health centers (FQHCs). All value sets utilized in our measure rely on standardized coding systems and are published on VSAC.
For more information on the feasibility of the Contraceptive Care Screening eCQM, see Section 3 Feasibility. To review our reliability and validity analyses methods and results, see Section 4, Scientific Acceptability.
Numerator
The numerator includes patients in the denominator who were asked the SINC question during the measurement period and had at least one documented response.
The numerator includes patients in the denominator who were asked the SINC question during the measurement period and had at least one documented response. All data elements necessary to calculate the numerator are defined within the value set named Self Identified Need for Contraception (SINC, OID 2.16.840.1.113883.6.1) in the Value Set Authority Center (VSAC). The measure’s specification was developed in CMS’ Measure Authoring Development Integrated Environment (MADiE) system and uses direct reference codes for the SINC Screening question and its multiple response options. This eCQM specification utilizes Clinical Quality Language (CQL) and Quality Data Model (QDM 5.6).
Denominator
Patients assigned female at birth aged 15-44 years who had a qualifying encounter during the measurement period; includes patients who have not had a live birth delivery and are not eligible for postpartum contraception, who are not anatomically infecund, and who have not undergone female sterilization.
The measure denominator includes patients assigned female at birth aged 15-44 who had a qualifying encounter (QE) during the measurement period. Age is calculated with the start of the measurement period as an anchor date.
The measurement period is a single calendar year. The measure is patient-based and calculated at the facility level of analysis. All data elements necessary to calculate this denominator are defined within the active value sets in the Value Set Authority Center (VSAC) and listed below:
- Assigned female at birth is defined with a direct reference code for Female in the value set ONC Administrative Sex (OID 2.16.840.1.113762.1.4.1)
- QEs are defined by the following value sets:
- Home Healthcare Services (OID: 2.16.840.1.113883.3.464.1003.101.12.1016)
- Office Visit (OID 2.16.840.1.113883.3.464.1003.101.12.1001)
- Preventive Care Services Established Office Visit, 18 and Up (OID: 2.16.840.1.113883.3.464.1003.101.12.1025)
- Preventive Care Services Initial Office Visit, 18 and Up (OID 2.16.840.1.113883.3.464.1003.101.12.1023)
- Preventive Care Services, Initial Office Visit, 0 to 17 (OID 2.16.840.1.113883.3.464.1003.101.12.1022)
- Preventive Care, Established Office Visit, 0 to 17 (OID 2.16.840.1.113883.3.464.1003.101.12.1024)
- Telephone Visits (OID 2.16.840.1.113883.3.464.1003.101.12.1080)
- Virtual Encounter (OID 2.16.840.1.113883.3.464.1003.101.12.1089)
A single code from the QE value sets documented during the measurement period counts as a QE.
Exclusions
Patients are excluded from the denominator if they had a live birth and are eligible for postpartum contraception during the measurement period (i.e., had a prenatal care visit plus a documented live birth delivery date or documented estimated delivery date without a non-live birth event between 3 months prior to the measurement period and 9 months into the measurement period), are anatomically infecund (i.e., due to removal of uterus and/or both ovaries), or have had female sterilization (i.e., use permanent contraception).
The measurement period is one calendar year, and this measure uses two years of data: the year prior to the measurement period, and the measurement period.
Patients who are excluded from the denominator meet one of the following criteria:
1) Had a live birth making them eligible for postpartum contraception in the measurement period: Those who had a prenatal care visit in the year prior to the measurement period through the first 9 months of the measurement period (i.e., 1/1/XX-1 through 9/30/XX) with a documented live birth delivery date, or a documented estimated delivery date (EDD) between 3 months prior to the measurement period and 9 months into the measurement period (i.e., 10/1/XX-1 through 9/30/XX), provided that those with EDD only did not have a documented ectopic pregnancy, intrauterine fetal demise, early pregnancy loss, or abortion (i.e., non-live birth event)
2) Are anatomically infecund: those with documentation of anatomical infecundity due to removal of uterus and/or bilateral ovaries during year prior to the measurement period and through the measurement period (i.e., 1/1/XX-1 through 12/31/XX)
3) Have had female sterilization or had a sterilization during the measurement period: those with a bilateral tubal ligation or bilateral salpingectomy in year prior to measurement period through measurement period (i.e., 1/1/XX-1 through 12/31/XX)
All data elements necessary to calculate the denominator exclusions are defined within value sets active in the Value Set Authority Center (VSAC) and listed below:
Patients eligible for postpartum contraception are represented by
• Live Birth Delivery Procedures (OID 2.16.840.1.113762.1.4.1166.177);
• Direct reference code “Date and time of obstetric delivery" (LOINC Code 93857-1);
• Direct reference code “Delivery date Estimated” (LOINC Code 11778-8);
• Prenatal Care Bundle Visits (OID 2.16.840.1.113762.1.4.1166.205);
• Prenatal Care Specific Visits (OID 2.16.840.1.113762.1.4.1166.114);
• General Prenatal Care Visits (OID 2.16.840.1.113762.1.4.1166.135);
• Telephone Visits (OID 2.16.840.1.113883.3.464.1003.101.12.1080);
• Virtual Encounter (OID 2.16.840.1.113883.3.464.1003.101.12.1089);
• Pregnancy Related Diagnoses (OID 2.16.840.1.113762.1.4.1166.133)
• Non Live Birth Procedures (OID 2.16.840.1.113762.1.4.1166.137)
• Non Live Birth Diagnoses (OID 2.16.840.1.113762.1.4.1166.136)
Patients who are anatomically infecund are represented by:
• Infecund Not for Contraceptive Reasons ICD10CM (OID 2.16.840.1.113762.1.4.1166.97)
• Infecund Not for Contraceptive Reasons Procedures (OID 2.16.840.1.113762.1.4.1166.151)
• Infecund Not for Contraceptive Reasons SNOMED Findings (OID 2.16.840.1.113762.1.4.1166.96)
Patients who have had female sterilization are represented by:
• Female Sterilization Provision Procedures (OID 2.16.840.1.113762.1.4.1166.142)
• Sterilization SNOMED Findings (OID 2.16.840.1.113762.1.4.1166.109)
• Direct reference code “Encounter for female sterilization” (ICD-10-CM Code Z30.2)
• Direct reference code “Female sterilization” (LOINC Code LA27905-1)
• Direct reference code “Permanent implantable contraceptive intratubal occlusion device(s) and delivery system” (HCPCS Code A4264)
• Direct reference code “Tubal ligation status” (ICD-10-CM Code Z98.51)
Measure Calculation
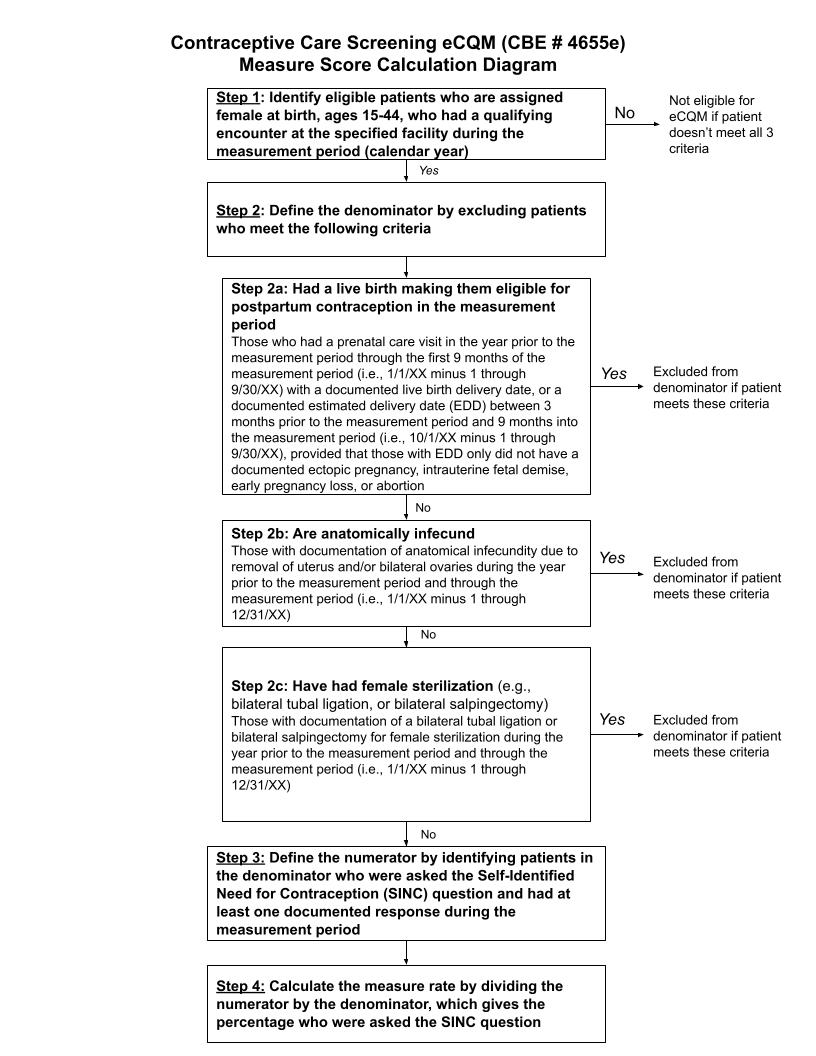
Step 1. Identify all patients who are female assigned at birth, ages 15-44 years who had a qualifying encounter at the specified facility during the measurement period (calendar year)
Step 2. Define the denominator by excluding patients assigned female at birth who:
- Had a live birth making them eligible for postpartum contraception in the measurement period: Those who had a prenatal care visit in the year prior to the measurement period through the first 9 months of the measurement period (i.e., 1/1/XX-1 through 9/30/XX) with a documented live birth delivery date, or a documented estimated delivery date (EDD) between 3 months prior to the measurement period and 9 months into the measurement period (i.e., 10/1/XX-1 through 9/30/XX), provided that those with EDD only did not have a documented ectopic pregnancy, intrauterine fetal demise, early pregnancy loss, or abortion (i.e., non-live birth event);
- Are anatomically infecund: those with documentation of anatomical infecundity due to removal of uterus and/or bilateral ovaries during year prior to the measurement period and through the measurement period (i.e., 1/1/XX-1 through 12/31/XX)
- Have had female sterilization (e.g., bilateral tubal ligation, or bilateral salpingectomy): Those with documentation of a bilateral tubal ligation or bilateral salpingectomy for female sterilization during the year prior to the measurement period and through the measurement period (i.e., 1/1/XX-1 through 12/31/XX)
Step 3. Define the numerator by identifying patients in the denominator who were asked the Self-Identified Need for Contraception (SINC) question and had at least one documented response during the measurement period
Step 4: Calculate the measure rate by dividing the numerator by the denominator, which gives the percentage who were asked the SINC question
{kind=link}
The measure is not stratified.
Not applicable – not based on sample
Measure Record
Point of Contact
Not Applicable
Christine Dehlendorf
San Francisco, CA
United States
Fei Dong
Far Harbor
Austin, TX
United States
Importance
Evidence
Access to high quality, patient-centered contraceptive care is essential for people to achieve their reproductive goals.
Achieving individual reproductive goals depends on being able to achieve or prevent pregnancy when and how a person wants (1). In 2015, based on National Survey of Family Growth (NSFG) data, only 47.9% of pregnancies were categorized as occurring as desired at the time for the individual (2). Contraceptive technology is key for those who want to prevent pregnancy, and the most commonly used contraceptive methods in the United States require contact with a health care provider (3). Moreover, access to sexual and reproductive healthcare has been associated with use of prescription contraceptive methods and contraceptive counseling has been linked to ongoing contraceptive use (4,5).
Barriers to access to contraceptive care exist.
Despite this need for contraceptive services, many people who do not want to become pregnant do not use contraception. Data from the NSFG, for example, found that of those at risk of an unintended pregnancy and who were sexually active, 18% were not using any form of contraception, and, of those, 84% did not want to become pregnant in the following two years (6). One contributor to these statistics is lack of access to contraceptive care. Within this analysis, among those who wanted to prevent pregnancy for at least 5 years, 19% reported that they were not using contraception because they could not access a method (6). More broadly, NSFG analyses find that only 46% of women at risk of unintended pregnancy receive contraceptive services in a year, with disparities by both race/ethnicity and age (with younger patients being less likely to receive contraceptive services) (7). Further, among ambulatory encounters with women of reproductive age in the United States, only 14% include any reproductive health services, including contraception (8).
Gaps in care access are not equitably experienced across demographic groups.
In one NSFG analysis of the 2006-2017 waves of data collection found that overall 18.3% of women of reproductive age received contraceptive counseling, and when looking at subgroups, found the Black and Latina heterosexual women had lower odds of receiving contraceptive counseling compared to white heterosexual women (with Latina sexual minority women having the lowest odds) (9). Additionally, changing policy environments have led to a decrease in contraceptive care access and increased barriers to care. A recent study used four waves of cross-sectional study data to look at changes in contraceptive care access in four states between 2021 and 2023 and found a four-percentage point increase in reported barriers to accessing contraceptive care between the time points (10). Moreover, ten percent of respondents who were not using a preferred contraceptive method named access barriers, including difficulty accessing a facility, as a reason (11). These barriers infringe upon individuals’ ability to access and use contraception, compromising their ability to achieve their reproductive goals.
Screening for contraceptive need can enhance access. One evidence-based strategy to enhance the ability of those who want contraceptive care to receive it is to ensure that patients accessing care for any reason are screened for contraceptive need, with integration of proactive screening for pregnancy prevention need being promoted by the Centers for Disease Control and Prevention and the American College of Obstetricians and Gynecologists (12,13). This is particularly relevant in the primary care context, in which many reproductive age women receive care (14) and in which competing priorities, including preventive health screening and chronic disease management, can interfere with attention to reproductive health needs. Standardized screening for contraceptive need can aid in ensuring that individual’s reproductive health needs are being met alongside these other key health needs; implementation of standardized reproductive needs screening has been shown to increase documentation of contraceptive care screening in health center settings (15). Additionally, ensuring contraceptive care screening is incorporated into diverse healthcare settings, including primary care, could help increase access to contraceptive counseling, as reported challenges to integrating contraceptive care into primary care include lack of provider counseling initiation due to factors including assumption about patient need and interest, and relying on the patient to initiate provision (16–19). Thus, implementation of standardized screening can complement other systems-level efforts, including provider training and use of patient decision support tools, to optimize contraceptive care (20). One study showed that standardized integration of reproductive health screening in a community health center setting led to a 24% increase in clinician counseling about contraception (8), ultimately expanding access to wanted contraceptive services.
Standardized screening for desire for contraceptive care must be implemented in a patient-centered manner with attention to the history and context of contraceptive care delivery. Standardized screening approaches must be patient-centered in order to ensure they optimize patient care experience. This is particularly true in the context of reproductive health care, which encompasses sensitive services that require attention to patient comfort in discussing personal issues. Further, it is essential to recognize that the provision of contraception care services has a fraught history in the United States, marked by targeted marketing of birth control to and forced sterilization of Black and Indigenous people of color, as well as people living on low-incomes and people with disabilities, motivated by the desire to curb the reproduction of these groups (21,22). Asking about contraception and pregnancy prevention in the healthcare setting carries the weight of this history. It is therefore critical that screening for contraceptive need is done in a manner that does not inadvertently reproduce harm by communicating a sense of expectation or pressure to use pregnancy prevention methods. This is particularly critical as even in current clinical practice, Black and Latina women have been documented to be more likely to be subjected to directive, non-patient-centered contraceptive and reproductive health care services (23–27). Several evidence-informed commentaries have highlighted the ways in which structures of power in health systems and care delivery, including how we ask individuals about their pregnancy prevention needs, entrenches inequities by stigmatizing the reproduction of certain groups, such people living on low incomes and people of color, and titrating their care and de-centering their needs (1,28,29). Person-centered approaches to contraceptive care screening must therefore work to re-center individual preferences, needs and values.
Literature on patient preferences for screening has highlighted that patients prefer to be asked about their reproductive health needs through service-bound questions. In one qualitative study, patients desired contraceptive counseling availability in primary care, provided that they engage in a manner that respects their autonomy and reproductive desires. To achieve this, they preferred a contraceptive care screening question that was open-ended, inclusive, and promoted autonomy, with a preference for a service-bound question akin to SINC (30). This finding was further tested and reinforced in a survey of over 1,000 federally qualified health center patients in New York (31).
The SINC screening question is therefore an evidence-based, person-centered approach to screening for contraceptive need. The SINC screening question was developed in response to this evidence for patient-centered approaches to screening and consists of a standardized question and response options in the LOINC code system. Developed through our engagement with Reproductive Justice consultants and industry stakeholders, this screening question asks patients for their desire for contraceptive services on the day of their visit. Building on the literature assessing how patients want to be asked about their reproductive needs, SINC takes a person-centered, service-bound approach that does not rely on assumptions about why patients are seeking contraception (28). SINC is aligned with the increasing attention to the need for respectful reproductive care by focusing on patients’ own assessment of their pregnancy prevention needs instead of basing assessment of contraceptive on assumptions about when and how people should become pregnant or use contraception. A standardized measure of self-identified contraceptive need provides an opportunity to hardwire patient-centered and reproductive autonomy focused workflows into the EHR that can facilitate patients getting their needs met. Throughout the development of this question and the response options, attention was paid to ensure that people’s own preferences and needs related to reproduction are recognized and respected. For example, by initiating the screening with a reference to the standardized nature of the question, we sought to prevent any perceived or real targeting of the reproductive choices of certain individuals or individuals from certain groups. We also carefully considered the ordering of the answer options so as not to infer that the most or only acceptable response was “I am already using contraception”. Implementation of this screening is designed to support reproductive autonomy and patient privacy, as well as decrease inequities in the provision of contraception services. For this reason, guidance is to ask patients of reproductive age SINC annually, creating access opportunity without undue pressure. Guidance also includes asking SINC to current prescription contraceptive users, recognizing that these individuals may want to switch or discontinue methods and should be provided with opportunity to discuss their contraceptive needs. Service-bound screening through the use of SINC therefore helps center patients in their own decision at the time of visit and enables them to meet their long-term reproductive goals, including using pregnancy prevention when desired, while protecting against provider and health system bias.
We emphasize that we have intentionally defined the specifications for this measure to be aligned with principles of patient-centeredness, as delineated in Providing Quality Family Planning Services: Recommendations of CDC and the U.S. Office of Population Affairs. (32). First, we have included patients who are currently using methods, as current users should still be screened annually, as they may be interested in changing or stopping methods or have questions about their method. This is particularly salient for individuals using long-acting reversible contraceptive (LARC), where removal is provider-dependent. The measure excludes individuals who receive prenatal care for a pregnancy that would make them eligible for postpartum contraception during the measurement period. Individuals who receive peripartum care have reproductive health needs that are distinct and temporally bound to the timing of their pregnancy and delivery (e.g., most pregnant individuals receive contraceptive counseling at visits occurring between 24 and 32 weeks of their pregnancy). Screening for contraceptive need during and directly following pregnancy is already well-incorporated into workflows and systems of care. One PRAMS assessment found that majority of women received prenatal (78%) and postpartum (86%) contraceptive counseling; 72% received both (33). As a result, the quality gap is not whether individuals are being screened for contraceptive need, but rather the quality of the contraceptive counseling itself. Therefore, standardized screening through SINC does not address a gap in care for these individuals. Utilizing SINC in place of current planning-based screening tools common in peripartum contraceptive counseling would increase the person-centeredness of screening and be aligned with reproductive autonomy, but requiring reporting of SINC in this time period has the potential to communicate undue pressure on the individual in the peripartum period, particularly among those who already formulated decisions early in pregnancy about their postpartum contraceptive use.
Before SINC no measure of patient desire for contraceptive services existed for consistent implementation across electronic health record (EHR) systems (note that One Key Question® (34), a proprietary question that assess desire for pregnancy in the next year, does not fulfill this need, in that it assesses future desires, rather than immediate need for services). Alternative approaches commonly used in assessing for contraceptive need use indirect methods of assessment, such as asking about future pregnancy desires. We recently published an evidence-informed commentary in Contraception that highlights that this approach is not patient-centered and does not reflect how many people think about pregnancy and pregnancy prevention. Namely, a pregnancy intention-based approach ignores the complexity of lived experience and feelings toward pregnancy and pregnancy prevention (28). Additionally, two studies tested one such approach, One Key Question®, alongside a measure of current desire for pregnancy prevention. These studies found that desire for future pregnancy or ambivalence about future pregnancy and desire for pregnancy prevention now were not always aligned – a sizable minority of those surveyed who wanted pregnancy in the next year wanted to prevent pregnancy now (35,36). Pragmatically that means that if employed as a screening tool, this or similar screening approaches will miss individuals who desire contraceptive services.
Measurement of SINC utilization will identify gaps in meeting patient needs and serve as the basis for quality improvement to enhance contraceptive care provision. Multiple commentaries have detailed how the use of performance measures related to contraceptive provision can improve the quality of contraceptive care and promote positive reproductive health outcomes (37–39). A measure of contraceptive screening is an essential addition to the ecosystem of contraceptive measures, providing a critical step in the pathway to contraceptive provision and use, as currently measured in CBE #2902, #2903, #2904, #3699e, and #3682e. Having SINC as the basis of this screening measures aligns with quality as defined by National Academy of Medicine (40) and is an effective and patient-centered approach to identifying those with a contraceptive need that is responsive to individual perspectives on reproduction and the history of harm enacted in the reproductive health care delivery system. The promise of this measure was recently emphasized in the CMS bulletin on family planning services, which stated that states could consider including SINC in their standard data collection to assess whether individuals are receiving respectful care and the family planning services and supplies they need (41). In addition, earlier this year the Human Resources and Services Administration (HRSA) announced a new requirement for federally qualified health centers to report the number of patients screened for contraception need using a standardized screening instrument (31). HRSA named SINC explicitly as an instrument to use to meet this requirement. The Office of Population Affairs also included SINC as an optional reporting element in FPAR 2.0 (data element 41) (32).
We emphasize that we have intentionally defined the specifications for this measure to be aligned with principles of patient-centeredness, as delineated in Providing Quality Family Planning Services: Recommendations of CDC and the U.S. Office of Population Affairs. (32). First, we have included patients who are currently using methods, as current users should still be screened annually, as they may be interested in changing or stopping methods or have questions about their method. This is particularly salient for individuals using long-acting reversible contraceptive (LARC), where removal is provider-dependent. The measure excludes individuals who receive prenatal care for a pregnancy that would make them eligible for postpartum contraception during the measurement period. Individuals who receive peripartum care have reproductive health needs that are distinct and temporally bound to the timing of their pregnancy and delivery (e.g., most pregnant individuals receive contraceptive counseling at visits occurring between 24 and 32 weeks of their pregnancy). Screening for contraceptive need during and directly following pregnancy is already well-incorporated into workflows and systems of care. One PRAMS assessment found that majority of women received prenatal (78%) and postpartum (86%) contraceptive counseling; 72% received both (33). As a result, the quality gap is not whether individuals are being screened for contraceptive need, but rather the quality of the contraceptive counseling itself. Therefore, standardized screening through SINC does not address a gap in care for these individuals. Utilizing SINC in place of current planning-based screening tools common in peripartum contraceptive counseling would increase the person-centeredness of screening and be aligned with reproductive autonomy, but requiring reporting of SINC in this time period has the potential to communicate undue pressure on the individual in the peripartum period, particularly among those who already formulated decisions early in pregnancy about their postpartum contraceptive use.
REFERENCES
1. Dehlendorf C, Akers AY, Borrero S, Callegari LS, Cadena D, Gomez AM, et al. Evolving the Preconception Health Framework: A Call for Reproductive and Sexual Health Equity. Obstet Gynecol. 2021 Feb 1;137(2):234–9.
2. Kost K, Zolna M, Murro R. Pregnancies in the United States by Desire for Pregnancy: Estimates for 2009, 2011, 2013, and 2015. Demography. 2023 Jun 1;60(3):837–63.
3. Daniels K, Abma JC. Current Contraceptive Status Among Women Aged 15-49: United States, 2017-2019. NCHS Data Brief. 2020 Oct;(388):1–8.
4. Lee JK, Parisi SM, Akers AY, Borrerro S, Schwarz EB. The Impact of Contraceptive Counseling in Primary Care on Contraceptive Use. J GEN INTERN MED. 2011 Jul;26(7):731–6.
5. Kavanaugh ML, Pliskin E. Use of contraception among reproductive-aged women in the United States, 2014 and 2016. F&S Reports. 2020 Sep;1(2):83–93.
6. Frederiksen BN, Ahrens K. Understanding the extent of contraceptive non-use among women at risk of unintended pregnancy, National Survey of Family Growth 2011-2017. Contracept X. 2020;2:100033.
7. Pazol K, Robbins CL, Black LI, Ahrens KA, Daniels K, Chandra A, et al. Receipt of Selected Preventive Health Services for Women and Men of Reproductive Age - United States, 2011-2013. MMWR Surveill Summ. 2017 Oct 27;66(20):1–31.
8. Bello JK, Rao G, Stulberg DB. Trends in contraceptive and preconception care in United States ambulatory practices. Fam Med. 2015 Apr;47(4):264–71.
9. Agénor M, Pérez AE, Wilhoit A, Almeda F, Charlton BM, Evans ML, et al. Contraceptive Care Disparities Among Sexual Orientation Identity and Racial/Ethnic Subgroups of U.S. Women: A National Probability Sample Study. J Womens Health (Larchmt). 2021 Oct;30(10):1406–15.
10. Kavanaugh ML, Friedrich-Karnik A. Has the fall of Roe changed contraceptive access and use? New research from four US states offers critical insights. Health Affairs Scholar. 2024 Feb 1;2(2):qxae016.
11. Kavanaugh ML, Hussain R, Little AC. Unfulfilled and method‐specific contraceptive preferences among reproductive‐aged contraceptive users in Arizona, Iowa, New Jersey, and Wisconsin. Health Services Research. 2024 Jun;59(3):e14297.
12. Johnson K, Posner SF, Biermann J, Cordero JF, Atrash HK, Parker CS, et al. Recommendations to improve preconception health and health care--United States. A report of the CDC/ATSDR Preconception Care Work Group and the Select Panel on Preconception Care. MMWR Recomm Rep. 2006 Apr 21;55(RR-6):1–23.
13. ACOG Committee Opinion No. 762: Prepregnancy Counseling. Obstetrics & Gynecology. 2019 Jan;133(1):e78–89.
14. Ranji U, Salganicoff A, Sobel L, Gomez I. Financing Family Planning Services for Low-income Women: The Role of Public Programs [Internet]. KFF; 2019 Oct [cited 2024 Jul 18]. Available from: https://www.kff.org/womens-health-policy/issue-brief/financing-family-p…
15. Shah SD, Prine L, Waltermaurer E, Rubin SE. Feasibility study of family planning services screening as clinical decision support at an urban Federally Qualified Health Center network. Contraception. 2019 Jan;99(1):27–31.
16. Akers AY, Gold MA, Borrero S, Santucci A, Schwarz EB. Providers’ Perspectives on Challenges to Contraceptive Counseling in Primary Care Settings. Journal of Women’s Health. 2010 Jun;19(6):1163–70.
17. Chuang CH, Hwang SW, McCall‐Hosenfeld JS, Rosenwasser L, Hillemeier MM, Weisman CS. Primary Care Physicians’ Perceptions of Barriers To Preventive Reproductive Health Care In Rural Communities. Perspect Sexual Reproductive. 2012 Jun;44(2):78–83.
18. Zephyrin L, Suennen L, Viswanathan P, Augenstein J, Bachrach D. TRansforming Primary Health Care for Women: Part 1: A Framework for Addressing Gaps and Barriers [Internet]. The Commonwealth Fund; 2020 Jul. Available from: https://www.commonwealthfund.org/sites/default/files/2020-07/Zephyrin_p…
19. Dunlop AL, Jack B, Frey K. National Recommendations for Preconception Care: The Essential Role of the Family Physician. The Journal of the American Board of Family Medicine. 2007 Jan 1;20(1):81–4.
20. Borrero S, Callegari L. Integrating Family Planning into Primary Care—a Call to Action. J GEN INTERN MED. 2020 Mar;35(3):625–7.
21. Stern AM. Sterilized in the name of public health: race, immigration, and reproductive control in modern California. Am J Public Health. 2005 Jul;95(7):1128–38.
22. Roberts D. Killing the Black Body. New York, NY: Penguin Random House; 1998.
23. Gomez AM, Wapman M. Under (implicit) pressure: young Black and Latina women’s perceptions of contraceptive care. Contraception. 2017 Oct;96(4):221–6.
24. Gomez AM, Fuentes L, Allina A. Women or LARC First? Reproductive Autonomy And the Promotion of Long-Acting Reversible Contraceptive Methods. Perspect Sex Repro H. 2014 Sep;46(3):171–5.
25. Oakley LP, Harvey SM, López-Cevallos DF. Racial and Ethnic Discrimination, Medical Mistrust, and Satisfaction with Birth Control Services among Young Adult Latinas. Womens Health Issues. 2018 Aug;28(4):313–20.
26. Logan RG, Vamos CA, Daley EM, Louis-Jacques A, Marhefka SL. Understanding young Black women’s socialisation and perceptions of sexual and reproductive health. Cult Health Sex. 2022 Dec;24(12):1760–74.
27. Higgins JA, Kramer RD, Ryder KM. Provider Bias in Long-Acting Reversible Contraception (LARC) Promotion and Removal: Perceptions of Young Adult Women. Am J Public Health. 2016 Nov;106(11):1932–7.
28. Dehlendorf C, Perry JC, Borrero S, Callegari L, Fuentes L, Perritt J. Meeting people’s pregnancy prevention needs: Let’s not force people to state an “Intention.” Contraception. 2024 Jul;135:110400.
29. Brandi K, Fuentes L. The history of tiered-effectiveness contraceptive counseling and the importance of patient-centered family planning care. American Journal of Obstetrics and Gynecology. 2020 Apr;222(4):S873–7.
30. Manze MG, Romero DR, Sumberg A, Gagnon M, Roberts L, Jones H. Women’s Perspectives on Reproductive Health Services in Primary Care. Fam Med. 2020 Feb 7;52(2):112–9.
31. Jones HE, Calixte C, Manze M, Perlman M, Rubin S, Roberts L, et al. Primary care patients’ preferences for reproductive health service needs assessment and service availability in New York Federally Qualified Health Centers. Contraception. 2020 Apr;101(4):226–30.
32. Gavin L, Moskosky S, Carter M, Curtis K, Glass E, Godfrey E, et al. Providing quality family planning services: Recommendations of CDC and the U.S. Office of Population Affairs. MMWR Recomm Rep. 2014 Apr 25;63(RR-04):1–54.
33. Zapata LB, Murtaza S, Whiteman MK, Jamieson DJ, Robbins CL, Marchbanks PA, et al. Contraceptive counseling and postpartum contraceptive use. American Journal of Obstetrics and Gynecology. 2015 Feb;212(2):171.e1-171.e8.
34. Power to Decide. One Key Question online [Internet]. Available from: https://powertodecide.org/one-key-question
35. Wingo E, Dehlendorf C. Lack of pregnancy intention or interest in pregnancy prevention now? How best to screen for desire for contraceptive care. Contraception. 2023 Oct 6;110303.
36. Congdon JL, Vittinghoff E, Dehlendorf C. Comparison of a person-centered pregnancy prevention question and One Key Question to assess postpartum contraceptive needs. Contraception. 2024 Jul;135:110465.
37. Gavin L, Frederiksen B, Robbins C, Pazol K, Moskosky S. New clinical performance measures for contraceptive care: their importance to healthcare quality. Contraception. 2017 Sep;96(3):149–57.
38. Gavin LE, Ahrens KA, Dehlendorf C, Frederiksen BN, Decker E, Moskosky S. Future directions in performance measures for contraceptive care: a proposed framework. Contraception. 2017 Sep;96(3):138–44.
39. Moniz MH, Gavin LE, Dalton VK. Performance Measures for Contraceptive Care: A New Tool to Enhance Access to Contraception. Obstetrics & Gynecology. 2017 Nov;130(5):1121–5.
40. Institute of Medicine (US) Committee on Quality of Health Care in America. Crossing the Quality Chasm: A New Health System for the 21st Century [Internet]. Washington (DC): National Academies Press (US); 2001 [cited 2022 May 20]. Available from: http://www.ncbi.nlm.nih.gov/books/NBK222274/
41. Tsai Da. CMCS Informational Bulletin: Medicaid Family Planning Services and Supplies: Requirements and Best Practices [Internet]. 2024 [cited 2024 Sep 5]. Available from: https://www.medicaid.gov/federal-policy-guidance/downloads/cib08082024…
Measure Impact
If implemented, we anticipate an increase in contraceptive need screening in diverse healthcare settings. There are gaps in the provision of contraceptive care, despite recommendations from multiple professional organizations for universal screening (6–8). As a result of increased screening, individuals will face decreased barriers and greater access opportunities to desired contraceptive methods, including access in their preferred settings, such as primary care. Ultimately, this will mean more individuals who want contraception will use their preferred method (intermediate outcome). Uptake and implementation of SINC also serves to optimize the currently endorsed Contraceptive Use eCQMs (3699e) and LARC provision eCQM (sub-measure 3699e). SINC is used to define the denominator of those measures by excluding those patients who have a recorded “No” response to SINC in a calendar year. By defining the denominator as people who self-identify as needing contraceptive services, CBE #3682e shifts focus to people’s reproductive health needs as they define them. Implementing the Contraceptive Care Screening eCQM process measure will optimize the intermediate outcome measure of contraceptive use, resulting in quality improvement initiatives that help health care organizations better meet patients’ needs by increasing patient-centered access to contraception in a wider range of settings, a step towards the goal of reproductive autonomy and well-being for all.
Implementation of the Contraceptive Care Screening eCQM will also promote use of SINC as the preferred screening tool for contraceptive care need, increasing effectiveness, patient-centeredness, and efficiency of screening. Other commonly used screening approaches rely on future pregnancy planning desires, which can miss individuals who want contraception at the time of visit (62,63). SINC, in contrast, directly asks patients about their contraceptive service needs. This also is aligned with how patients want to be asked about their reproductive health needs (16,61). Implementing the Contraceptive Care Screening eCQM would thus lead to more patient-centered, effective, and thus higher quality, contraceptive care workflows.
Screening for contraceptive need presents little risk of adverse events. The primary risk of contraceptive screening is generating undue pressure on individuals to use contraception, especially given the long history of forced or coerced reproductive control of people of color and people living on low incomes in the U.S. (9,56,60). However, the wording of the SINC screening tool was developed in collaboration with Reproductive Justice experts to ensure its phrasing was not coercive and aligned with literature from patients about how they want to be asked about their reproductive health needs, and it was collectively determined that annual screening met the balance of screening for need without over-screening in a way that could induce pressure (31). Additionally a universal, standardized approach to contraceptive care screening protects against targeting of specific populations. Thus, risk of coercion was intentionally considered and minimized in the creation of SINC and its associated implementation guidance and the risk is extremely low. Given the minimal risks and the benefit of addressing a key health services gap, net impact of implementation is positive and justified.
We recognize that sustainability matters and that efforts to implement new measures should be cognizant of increased resource burden on the system. As the SINC question is designed to be implemented in standard clinical workflows and can be extracted from the EHR, we do not anticipate a cost burden from the implementation of this measure. In addition, we note that the measure should not be evaluated based on its potential to decrease costs. Rather, the goal is to center people’s positive reproductive outcomes as defined by individuals themselves and to advance care pathways that meet their needs. Evaluating from a cost-saving lens would suggest that the healthcare system has a stake in whether individuals become pregnant or not, compromising person-centeredness and reproductive autonomy.
REFERENCES
1. Johnson K, Posner SF, Biermann J, Cordero JF, Atrash HK, Parker CS, et al. Recommendations to improve preconception health and health care--United States. A report of the CDC/ATSDR Preconception Care Work Group and the Select Panel on Preconception Care. MMWR Recomm Rep. 2006 Apr 21;55(RR-6):1–23.
2. ACOG Committee Opinion No. 762: Prepregnancy Counseling. Obstetrics & Gynecology. 2019 Jan;133(1):e78–89.
3. Bello JK, Rao G, Stulberg DB. Trends in contraceptive and preconception care in United States ambulatory practices. Fam Med. 2015 Apr;47(4):264–71.
4. Congdon JL, Vittinghoff E, Dehlendorf C. Comparison of a person-centered pregnancy prevention question and One Key Question to assess postpartum contraceptive needs. Contraception. 2024 Jul;135:110465.
5. Wingo E, Dehlendorf C. Lack of pregnancy intention or interest in pregnancy prevention now? How best to screen for desire for contraceptive care. Contraception. 2023 Oct 6;110303.
6. Manze MG, Romero DR, Sumberg A, Gagnon M, Roberts L, Jones H. Women’s Perspectives on Reproductive Health Services in Primary Care. Fam Med. 2020 Feb 7;52(2):112–9.
7. Jones HE, Calixte C, Manze M, Perlman M, Rubin S, Roberts L, et al. Primary care patients’ preferences for reproductive health service needs assessment and service availability in New York Federally Qualified Health Centers. Contraception. 2020 Apr;101(4):226–30.
8. Brandi K, Fuentes L. The history of tiered-effectiveness contraceptive counseling and the importance of patient-centered family planning care. American Journal of Obstetrics and Gynecology. 2020 Apr;222(4):S873–7.
9. Borrero S, Schwarz EB, Creinin M, Ibrahim S. The Impact of Race and Ethnicity on Receipt of Family Planning Services in the United States. Journal of Women’s Health. 2009 Jan;18(1):91–6.
10. Roberts D. Killing the Black Body. New York, NY: Penguin Random House; 1998.
11. Dehlendorf C, Perry JC, Borrero S, Callegari L, Fuentes L, Perritt J. Meeting people’s pregnancy prevention needs: Let’s not force people to state an “Intention.” Contraception. 2024 Jul;135:110400.
There are very few validated measures pertaining to reproductive healthcare, and even fewer for contraceptive care specifically. As such, there are no existing measures which address the healthcare need that our proposed eCQM does: whether patients are screened for contraceptive needs at least once per year. Existing contraceptive care measures, such as the OPA-stewarded Contraceptive Care measures (CBE #2902, #2903, and #2904) estimate the percentage of women ages 15-44 years provided a most or moderately effective method of contraception in two populations in this age range: postpartum women and all fecund women. These claims-based measures do not measure whether people who actually want contraception are receiving it. In response to this shortcoming, UCSF created the Contraceptive Use eCQMs for postpartum (#3682e) and non-postpartum (#3699e) patients. These measures evaluate contraceptive use among patients who express interest in receiving services, as identified through the SINC screening question, offering a clearer assessment of access for those desiring services. UCSF’s contraceptive use eCQMs were endorsed by NQF in December 2022 and will be due for maintenance with PQM in 2026.
While the claims-based Contraceptive Care measures and the Contraceptive Use eCQMs assess contraceptive use and provision, they do not provide data on the percentage of patients screened within a year for contraceptive need, which is a critical process measure on the pathway to meeting people’s reproductive needs. The Contraceptive Care Screening eCQM therefore adds an additional dimension in the measure of quality in the care pathway. These measures are further augmented by the CBE patient-reported outcome performance measure, the Person-Centered Contraceptive Counseling measure (CBE #3543), that assesses the quality of contraceptive counseling received. Ideally these measures would be used together, as part of an ecosystem of contraceptive care quality measures.
Contraception is a reproductive health technology relevant to many individuals and families throughout the life course. It can help enable individuals to build families and exercise reproductive autonomy aligned with their desires, preferences, values, and circumstances. Further, use of this technology is widespread; many patients who want to prevent pregnancy use contraceptive services to do so. Research shows desire to avoid pregnancy is strongly associated with contraceptive use (1–3) and use is prevalent; from 2015-2019, 26 million women received a contraceptive service in the United States (4). The most commonly used contraceptive methods in the United States require contact with a health care provider (5). Increased screening for contraceptive need (process outcome) resulting in increased access to and use of preferred contraceptive methods (intermediate outcome) will better meet patients’ needs by increasing patient-centered access to contraception, a step towards the goal of reproductive autonomy and well-being for all (long-term outcome).
The SINC was designed as a patient-centered approach responsive to patient preferences of how they would like to be asked about reproductive health service needs. Studies have highlighted that patients prefer to be asked about their reproductive health needs through service-bound questions. In one qualitative study, patients desired contraceptive counseling availability in primary care, provided that their care team engaged in a manner that respects their autonomy and reproductive desires. To achieve this, they preferred a contraceptive care screening question that was open-ended, inclusive, and promoted autonomy, in particular a service-bound question akin to SINC (6). This finding was further tested and reinforced in a survey of over 1,000 federally qualified health center patients in New York (7). SINC was developed through our engagement with Reproductive Justice thought leaders, patient advisors, and industry stakeholders to ensure the phrasing and approach resonated with patients and would not inadvertently pressure patients (8). The screening question language and response options were crafted intentionally and iteratively with patient and community input. These groups overall supported the development and utilization of this measure in clinical care and provided critical input for optimization of the SINC. PCRHP’s Patient Stakeholder Group – a group of young people of reproductive age who have accessed reproductive health services – uplifted the importance of the ability to opt out of receiving counseling through intentional inclusion of answer options such as “I am here for something else”. Further, they supported efforts to ensure the phrasing was succinct and interpretable for patients. Similarly, review by community groups, including the National Birth Equity Collaborative, provided input into wording and implementation guidance. Ultimately, the SINC screening tool takes a person-centered, service-bound approach that does not rely on assumptions about why patients are seeking contraception.
Moreover, research has shown that patients support integration of reproductive health screening into routine healthcare screenings as it streamlines access to contraceptive services and fulfills their reproductive health needs in the context of their whole health care (7,9,10). Implementing this performance measure will better meet patients’ needs by increasing patient-centered access to contraception in a wider range of settings.
REFERENCES
1. Samari G, Foster DG, Ralph LJ, Rocca CH. Pregnancy preferences and contraceptive use among US women. Contraception. 2020 Feb;101(2):79–85.
2. Rocca CH, Smith MG, Hale NL, Khoury AJ. Ranges of pregnancy preferences and contraceptive use: Results from a population‐based survey in the southeast United States. Perspect Sexual Reproductive. 2022 Sep;54(3):90–8.
3. Stulberg DB, Datta A, White VanGompel E, Schueler K, Rocca CH. One Key Question® and the Desire to Avoid Pregnancy Scale: A comparison of two approaches to asking about pregnancy preferences. Contraception. 2020 Apr;101(4):231–6.
4. Frost JJ, Mueller J, Pleasure ZH. Trends and Differentials in Receipt of Sexual and Reproductive Health Services in the United States: Services Received and Sources of Care, 2006–2019 [Internet]. Guttmacher Institute; 2021 Jun [cited 2024 Sep 10]. Available from: https://www.guttmacher.org/report/sexual-reproductive-health-services-i…
5. Daniels K, Abma JC. Current Contraceptive Status Among Women Aged 15-49: United States, 2017-2019. NCHS Data Brief. 2020 Oct;(388):1–8.
6. Manze MG, Romero DR, Sumberg A, Gagnon M, Roberts L, Jones H. Women’s Perspectives on Reproductive Health Services in Primary Care. Fam Med. 2020 Feb 7;52(2):112–9.
7. Jones HE, Calixte C, Manze M, Perlman M, Rubin S, Roberts L, et al. Primary care patients’ preferences for reproductive health service needs assessment and service availability in New York Federally Qualified Health Centers. Contraception. 2020 Apr;101(4):226–30.
8. Dehlendorf C, Perry JC, Borrero S, Callegari L, Fuentes L, Perritt J. Meeting people’s pregnancy prevention needs: Let’s not force people to state an “Intention.” Contraception. 2024 Jul;135:110400.
9. Becker D, Klassen AC, Koenig MA, LaVeist TA, Sonenstein FL, Tsui AO. Women’s Perspectives on Family Planning Service Quality: An Exploration of Differences by Race, Ethnicity and Language. Perspectives on Sexual and Reproductive Health. 2009 Sep;41(3):158–65.
10. Miles C, Weidner A, Summit AK, Thomson CJ, Zhang Y, Cole AM, et al. Patient opinions on sexual and reproductive health services in primary care in rural and urban clinics. Contraception. 2022 Oct;114:26–31.
Performance Gap
To assess variation of our proposed eCQM in the ambulatory primary care setting, we implemented and tested the Contraceptive Care Screening eCQM in nine Community Health Centers (CHCs) within two health care-controlled networks (HCCNs): HCCN 1 and HealthEfficient. HCCN 1 CHCs operate in states in the Midwest and West coast of the United States, while HealthEfficient CHCs are in the Northeast region of the country. We used the following data sets from each HCCN to provide measure scores and descriptive statistics for the scores at the facility (CHC) and clinician group/practice (site) levels of analysis in the most recent measurement period (2023).
(1) HCCN 1. The HCCN 1 dataset comprised all female clients aged 15-44 years from 17 outpatient sites nested in 6 CHCs in 2023.
(2) HealthEfficient. The HealthEfficient dataset comprised all female clients aged 15-44 years from 6 outpatient sites nested in 3 CHCs in 2023.
For the purposes of this application, UCSF suggests that the CHC and outpatient site be considered proxies for the facility and clinician group/practice levels of analysis respectively, since the outpatient sites operate as different locations of the same CHC.
Across the 6 facilities within HCCN 1, the overall performance score was 38.8%. The highest performing facility asked 82.1% of its eligible patients (n=19,723) the SINC Screening question; the lowest performing facility only asked 0.1% of eligible patients SINC. The overall performance score among the 3 facilities within HealthEfficient was 30.1%, while the percentage of eligible patients (n=4,405) asked the SINC question with a documented response ranged from 16.9 to 49.0%.
At the clinician group/practice (nested within CHC) level of analysis in both HCCN 1 and HealthEfficient, the lowest performing group/practice did not ask SINC of any eligible patients (0.0%) during the measurement period. The highest performing HCCN 1 group/practice asked 98.9% of eligible patients the SINC Screening question. Among HealthEfficient clinician groups/practices, the maximum measure score was 51.2%.
Our implementation and testing of the Contraceptive Care Screening eCQM in these nine facilities provide evidence of an existing performance gap for this measure in the primary care setting, given the variation in performance scores across facilities and clinician groups/practices within each HCCN. The facilities included in our analysis also participated in Innovating Contraceptive Care in Community Health Centers (ICC in CHCs), which was a quality improvement (QI) initiative to improve the contraceptive services they offer. This project provided CHCs with resources to effectively incorporate the Contraceptive Care Screening eCQM for the first time, including customized technical assistance sessions with UCSF and monthly learning community (LC) videoconference meetings for clinical and health information technology (HIT) staff. Our two HCCN partners first used the Contraceptive Care Screening question in early 2021. In both HCCNs, the percentage of encounters with a recorded SINC response increased during the active QI project period (which ended in summer 2023), indicating that room for improvement for this eCQM exists and that there is responsiveness to quality improvement efforts. In HCCN 1, the percentage of encounters with a documented SINC response was 0.3% across ICC-participating groups/practices in May 2021; in June 2023, this percentage increased to 9.9%. In HealthEfficient ICC participating groups/practices, the percentage of encounters with a recorded SINC response was 7.8% May 2021; in June 2023, it was 23.6%.
All tables contained in attachments uploaded under 2.4a
Care Gaps
Closing Care Gaps
The Self-Identified Need for Contraception screening question (SINC) was intentionally developed using a racial justice and health equity lens. The question was created to meet patients’ reproductive health needs while centering their autonomy and preferences (1). Our team collaborated with reproductive justice experts, Drs. Joia Crear-Perry and Jamila Perritt, to ensure this screening tool was patient-centered and did not replicate systems of oppression. Preconceived notions or stigma around reproductive healthcare can be reduced by normalizing screening all eligible patients for their contraceptive needs.
Routine screening for contraceptive needs has the potential to close barriers to accessing contraceptive care, particularly among group who may have limited access to healthcare. Black and Latinx patients report lower utilization of prescription contraceptive methods than their white counterparts (2,3). Therefore, the use of the Contraceptive Care Screening eCQM, which assesses the extent to which SINC is being utilized, provides an assessment of how frequently patients are having their contraceptive needs assessed. This will allow for the identification and improvement of gaps and inequities in this care.
While facing barriers to access, people of color and low-income communities also report experiencing pressure from clinicians to use contraception, particularly long-acting reversible contraception (LARC) (4–7). SINC gives agency back to patients, to choose whether they’d like to discuss contraception that day, whether they’d like to talk about it at their next visit, or if they never want to talk about it with this care team. Further, other methods of screening for contraceptive need triangulate need through a pregnancy intention framework. Studies show pregnancy intention-focused screening questions are not relevant to all patients (8), as a planning paradigm does not resonate with many patients. Use of a service needs question can help patients meet their needs at the time of their visit, rather than making assumptions about a what a person wants. Therefore, the Contraceptive Care Screening eCQM accomplishes the goal of assessing the extent of screening for contraceptive need in a manner that is patient-centered and responsive to existing inequities.
In addition to racial/ethnic inequities, it is important to consider the health care experiences of LGBTQIA+ patients, who may want to use contraception but are missed due to underlying assumptions about sexual activity and/or risk of pregnancy. LGBTQIA+ patients are less likely to receive contraceptive counseling (9). Asking a service needs question of all eligible patients could help correct this disparity by not making assumptions about sexual behavior or family formation context, ultimately connecting people who want contraception with the services they desire. Thus, the Contraceptive Care Screening eCQM also has the potential to advance equity in care for LGBTQIA+ patients.
REFERENCES
1. Person-Centered Reproductive Health Program [Internet]. [cited 2024 Jul 18]. Self-Identified Need for Contraception (SINC). Available from: https://pcrhp.ucsf.edu/sinc
2. Grady CD, Dehlendorf C, Cohen ED, Schwarz EB, Borrero S. Racial and ethnic differences in contraceptive use among women who desire no future children, 2006–2010 National Survey of Family Growth. Contraception. 2015 Jul;92(1):62–70.
3. Murray Horwitz ME, Pace LE, Ross-Degnan D. Trends and Disparities in Sexual and Reproductive Health Behaviors and Service Use Among Young Adult Women (Aged 18-25 Years) in the United States, 2002-2015. Am J Public Health. 2018 Nov;108(S4):S336–43.
4. Gomez AM, Wapman M. Under (implicit) pressure: young Black and Latina women’s perceptions of contraceptive care. Contraception. 2017 Oct;96(4):221–6.
5. Higgins JA, Kramer RD, Ryder KM. Provider Bias in Long-Acting Reversible Contraception (LARC) Promotion and Removal: Perceptions of Young Adult Women. Am J Public Health. 2016 Nov;106(11):1932–7.
6. Dehlendorf C, Anderson N, Vittinghoff E, Grumbach K, Levy K, Steinauer J. Quality and Content of Patient-Provider Communication About Contraception: Differences by Race/Ethnicity and Socioeconomic Status. Womens Health Issues. 2017 Oct;27(5):530–8.
7. Oakley LP, Harvey SM, López-Cevallos DF. Racial and Ethnic Discrimination, Medical Mistrust, and Satisfaction with Birth Control Services among Young Adult Latinas. Womens Health Issues. 2018 Aug;28(4):313–20.
8. Jones HE, Calixte C, Manze M, Perlman M, Rubin S, Roberts L, et al. Primary care patients’ preferences for reproductive health service needs assessment and service availability in New York Federally Qualified Health Centers. Contraception. 2020 Apr;101(4):226–30.
9. Agénor M, Pérez AE, Wilhoit A, Almeda F, Charlton BM, Evans ML, et al. Contraceptive Care Disparities Among Sexual Orientation Identity and Racial/Ethnic Subgroups of U.S. Women: A National Probability Sample Study. J Womens Health (Larchmt). 2021 Oct;30(10):1406–15.
Feasibility
Feasibility
Background
In our Innovating Contraceptive Care in Community Health Centers (ICC in CHCs) quality improvement (QI) initiative from 2020-2023, we implemented and measured the Contraceptive Care Screening eCQM in the EHR for 23 locations within nine Community Health Centers (CHCs), nested within two health-center controlled networks (HCCNs). Thus, the eCQM was tested and implemented in two different electronic health records (EHR) systems: HCCN 1 utilizes its customized version of Epic, and HealthEfficient uses eClinicalWorks (eCW). Our QI initiative also included one additional CHC that implemented the data element into their AthenaOne EHR system. We excluded this additional CHC from measure testing because we do not have access to their data.
Availability of data elements
The Contraceptive Care Screening eCQM requires availability of the SINC data element (aka Contraceptive Care Screening question) in EHR systems to allow for identification of client’s desire for contraceptive services in a patient-centered way.
With respect to implementation of the SINC data element, as described UCSF has worked with ten CHCs using three different EHR systems (eCW, Epic, AthenaOne). In these instances, EHR changes were able to be implemented in about three months in collaboration with clinical and vendor teams. The implementation burden depends on the change process for the EHR at the health system to embed the SINC data element into the relevant EHR template so that care teams can use SINC. HCCN 1 uses its customized version of Epic, a centrally managed EHR system, and easily implemented the Contraceptive Care Screening question across the ICC-participating CHCs. In HealthEfficient, each CHC uses eCW and implemented SINC at the individual ICC-participating sites; this de-centralized process required more coordination and time. During the final meeting for ICC in CHCs, one CHC using Epic stated, “(HCCN 1) did a phenomenal job with our SINC question (and) made it so user-friendly for our clinicians”. A CHC in HealthEfficient at the same meeting reported, “It was challenging to get the SINC implemented into our EMR; we use eCW and also train the staff, and (it was) more so a resource challenge, finding the time and staff to distribute the information about the changes.” In contrast, a different CHC in HealthEfficient, noted that implementing SINC screening into their EHR system facilitated their QI activities and stated, “I think that what made it easy for me … is that [the HIT staff] had already incorporated the [SINC] questions into our eCW. So it was something that was already running.” Most systems, from our experience, are able to implement the EHR template changes in about 3 months, with some systems requiring less time. We note that, in addition to the systems that implemented SINC as part of QI learning collaborative, clinical sites across the country have begun to implement and use this data element since it was made available as a LOINC code in August 2021, indicating the feasibility of this implementation. This includes Planned Parenthood Federation of America, which includes SINC as its Medical Standard and Guidelines as an approach to assessing reproductive needs, and sites affiliated with Upstream USA, including Cambridge Health Alliance.
Feasibility scorecard results
Our HCCN data partners completed the feasibility scorecards for the Contraceptive Care Screening eCQM to provide feedback on the measure and its calculation in their respective EHR systems (see the attached file named 4655e_PQM_ecqm_feasibility_scorecard_ HCCNs_508.xlsx”). The HCCNs evaluated a total of 40 data elements specified in our measure.
HealthEfficient indicated that 15% of the eCQM data elements scored 0 in the Data Availability feasibility domain (i.e., data are readily available in a structured format), 20% scored 0 in the Data Accuracy domain (i.e., information contained in the data is correct), 30% scored 0 in the Data Standards domain (i.e., data element is coded using a nationally accepted terminology standard and mapped to the QDM), and 38% scored 0 in the Workflow domain (i.e., extent to which data element capture impacts the workflow for the user). In contrast, HCCN 1 reported that 5-10% of eCQM data elements scored 0 for availability, accuracy, and standards, while 13% scored 0 for workflow. The HCCN data partners provided their solutions to address the Contraceptive Care Screening eCQM elements that did not achieve 100% across the four feasibility domains (see the tabs named, “Feasibility Plan” in the attached scorecard).
Recognizing that different EHR systems use multiple combinations of code systems, the Contraceptive Care Screening eCQM includes several terminologies that define the measure’s data elements to facilitate measure use and calculation, even if one code system is excluded. For example, the value sets that define anatomically infecund (i.e., infecundity due to removal of a patient’s uterus and/or both ovaries) include codes from ICD-10-CM, CPT, and SNOMED CT; thus, a CHC using at least one of these three value sets can still provide this data element. Both HCCNs had data elements that scored 0 in at least one of the four feasibility domains because the participating CHCs do not routinely offer services related to the data elements for live birth delivery, even if the partners’ EHR systems contain structured fields in which the information can reside. HealthEfficient had 15 data elements scoring 0 for the Workflow domain while HCCN 1 had five elements scoring 0 for Workflow, indicating that these elements are not routinely collected during clinical care. Furthermore, neither HCCN uses SNOMED CT code system in their EHR, which resulted in 0s for the Data Availability and Data Standards domains for SNOMED eCQM data elements.
Our proposed eCQM also utilizes definitions that include more than one type of health care service variable or field, allowing flexibility to primary care CHCs that do not offer all health care services but want to implement the measure. For example, the Contraceptive Care Screening eCQM defines qualifying encounters (QEs) as having a single code among eight different value sets. HealthEfficient does not offer the services defined by one QE code set (Home Healthcare Services) but offers the others as part of its primary care services; thus, HealthEfficient can still identify eligible patients who have QEs. Another example is that the eCQM allows for use of Estimated Delivery Date (EDD) when Live Birth Delivery Date is unavailable or missing from a patient’s record. Although our partners reported in the feasibility scorecard that Live Birth Delivery Date may not often be reported (because CHCs do not offer labor and delivery services), the EDD data element may be recorded for patients visiting CHCs for prenatal care services, making it available in both HCCNs’ EHR systems and for eCQM calculation.
Finally, the new SINC data element was initially not integrated into the EHR systems of the nine CHCs, but all facilities ultimately implemented it to assess contraceptive needs and to calculate the Contraceptive Care Screening eCQM. Unlike HCCN 1, which easily implemented SINC in its centrally-managed EHR system across their ICC-participating CHCs, HealthEfficient had to implement the SINC question and response options in their EHR for each participating CHC as separate processes over a longer time period. Thus, HealthEfficient reported in its scorecard that SINC is not routinely collected as part of regular clinical workflow. While one HealthEfficient CHC reported a smooth implementation of SINC use, the other CHCs found it more challenging to add the new element. Both HCCN 1 and HealthEfficient CHCs have maintained their use of SINC in primary care visits after the end of ICC in CHCs and expanded SINC use to additional clinician groups/practices that did not originally participate in our QI initiative.
Estimates of the costs or burden of Contraceptive Care Screening eCQM implementation
To implement SINC in partner EHR systems, our partner HCCNs changed their primary care EHR template to include the SINC question and its response options as structured fields. The EHR system programmers and analysts bore the burden of mapping EHR data required for the measure to the eCQM concepts according to the CHCs’ regular clinical workflows for the purposes of calculating and reporting the measure rates. After implementation, we estimate that data entry by clinical staff will require a minute or less to conduct. The SINC question and its response options are also specified in the LOINC code system and can be mapped as such for EHR systems that include LOINC.
With respect to clinical implementation, UCSF advocates for SINC to be included as part of a patient-centered primary care workflow, enhancing access to reproductive health services for those who need it. Therefore, the added time burden on the clinical workflow will be offset by enhanced quality of care. The SINC Screening question is estimated to require a minute or less to implement within the primary care workflow.
Data abstraction and measure reporting
The SINC data element resides within the clinical agency’s secure EHR system server. Each HCCN upholds the normal requirements to ensure that its EHR data elements, including SINC, are shared only with entities that have active data use agreements and the infrastructure to securely exchange Protected Health Information / Potentially Identifiable Information (PHI/PII).
During the ICC in CHCs project period, we worked with HCCN 1 and HealthEfficient to provide quality assurance (QA) checks of their datasets to calculate the Contraceptive Care Screening eCQM. Our QA involved confirming that the analysis datasets included both the required elements for measure calculation and all encounters occurring in two consecutive calendar years for patients assigned female at birth, ages 15-44. When questions about calculation arose, UCSF collaborated with the HCCN HIT staff to investigate and agree on a solution. One partner implemented a new EHR system in CHCs working on the QI initiative; in our QA, we helped the partner troubleshoot their new query system to obtain accurate encounter records to calculate the Contraceptive Care Screening eCQM.
UCSF’s two HCCN partners each completed chart reviews among a random sample of patients for the data element validity analysis (see Section 4.3 for full methodology and results). The partners encountered challenges extracting EHR data for a small number of Contraceptive Care Screening eCQM data elements: female sterilization, live birth delivery date, and estimated delivery date, which all refine the eCQM denominator. In our discussions with the partners about these elements, we learned that these elements may not be found in structured fields within the CHCs EHR in patients’ histories, in part because these events occurred in the past or at a different facility that delivers those services. The facilities and clinician groups/practices that participated in the chart reviews do not provide labor and delivery services and tubal ligation procedures. Furthermore, the internal means used to record these elements are not often mapped to standard terminologies, like SNOMED CT, LOINC, or other commonly used code systems like CPT or ICD-10-CM. For example, one HCCN partner utilizes custom, internal codes for female sterilization (e.g., tubal ligation) in their EHR system when this condition is reported by the patient, noted by a provider, and then entered into the patient’s record. Ideally, health systems that deliver inpatient health care services and connect patients’ inpatient and outpatient encounter records would document the prevalence of these conditions and services using standardized nomenclatures to inform providers and improve quality of care for patients.
Potential unintended consequences of availability of SINC Screening question in EHR systems
Availability of the SINC data element in EHR has the desired goal of facilitating patient-centered screening for contraceptive needs in a way that helps people receiving desired care and achieving their reproductive goals, as described in our logic model. To facilitate this practice change, UCSF developed a detailed implementation guide for the SINC Screening question into clinical workflows and corresponding EHR templates to identify patients’ preferences for reproductive health care in a person-centered manner. One possible unintended consequence with SINC implementation into their clinical workflow and EHR system is that primary care providers might feel compelled to ask their patients SINC more often. Asking the SINC Screening question too frequently might cause patients to feel pressure related to use of contraception, which results in care not centered on the person. For the ICC in CHCs initiative, we developed materials to support participating sites to have all the information they needed to implement SINC to provide person-centered health care services. During our monthly learning sessions, we also gave feedback to QI teams on their activities and results to re-emphasize our implementation guide and help participating sites. These resources will continue to be made available and best practices related to using SINC in a patient-centered manner will be emphasized in all dissemination activities.
Updates to value sets utilized in specification
To define live birth delivery, UCSF utilized an existing value set to draft the Contraceptive Care Screening eCQM in CMS’s Measure Authoring Development Integrated Environment (MADiE) website. In preparing for the feasibility assessment with our HCCN partners, we discovered that the value sets we initially selected for live birth delivery changed its status in the National Library of Medicine (NLM) Value Set Authority Center (VSAC) to “Not Maintained”. This status indicates that the value set is a previously published version meant for use in production systems at the time of its publication that has not been reviewed by its author or steward. To address this issue, we used a direct reference code to an active LOINC code and published our own value set that is actively maintained (Live Birth Delivery Procedures, OID 2.16.840.1.113762.1.4.1166.177).
Proprietary Information
Scientific Acceptability
Testing Data
Electronic health records (EHR) data from two networks were used for reliability and validity testing:
(1) Health-center controlled network (HCCN) 1. The HCCN 1 uses its customized Epic system and the dataset comprised all female clients aged 15-44 years from 17 outpatient sites (clinician groups/practices) nested in 6 Community Health Centers (facilities) located in Washington, Ohio, California, and Oregon in 2023.
(2) HealthEfficient. The HealthEfficient uses the eCW system and the dataset comprised all female clients aged 15-44 years from 6 outpatient sites (clinician groups/practices) nested in 3 Community Health Centers (facilities) located in Connecticut, New York, and New Jersey in 2023.
(1) HCCN 1. For reliability testing, the full dataset was used. For data element validity testing, we utilized data from a random sample of 150 female clients ages 15-44 who visited 8 sites in calendar year 2023. As it was not feasible for HCCN1 to do data element validity testing at all sites, these 8 sites were randomly selected to provide an overall assessment of the data validity in the network. The age distribution is comparable between the sample and the full dataset.
(2) HealthEfficient. For reliability testing, the full dataset was used. For data element validity testing, we utilized data from a random sample of 144 female clients ages 15-44 who visited 5 sites in calendar year 2023. One additional site was not selected because their data was not available for chart review. The age distribution is comparable between the sample and the full dataset.
Accountable Entity-Level Reliability
The measure was tested at the clinician group/practice-level and the facility-level for both data partners. Reliability testing used full denominator population in the datasets from HCCN 1 and HealthEfficient networks described above.
HCCN 1 includes 17 outpatient sites (clinician groups/practices) nested in 6 Community Health Centers (facilities) located in Washington, Ohio, California, and Oregon. HealthEfficient includes 6 outpatient sites (clinician groups/practices) nested in 3 Community Health Centers (facilities) located in Connecticut, New York, and New Jersey.
Data Element Validity
Eight sites from HCCN 1 and five sites from HealthEfficient provided data and the analysis was conducted using aggregated numbers across all sites for each network. A sample of 150 patients were randomly selected from the eight sites in HCCN 1 and 144 patients were randomly selected from the five sites in HealthEfficient.
See Section 4.2.3a. Tables 1-4 for tables of characteristics.
Reliability
Several methods have been suggested to assess the reliability of provider-level performance measures (1-3). These methods may focus on different facets of reliability such as consistency across time, consistency across raters or units, or variability at different levels of aggregation. The PQM has suggested a signal-to-noise approach as one way to evaluate measure reliability (4). For this application, reliability was estimated from a Beta-binomial model using parametric empirical Bayes methods. This method is better able to produce reliability estimates when the performance measures fall in the extreme ranges of the distribution (below 10% or above 90%), whereas the signal-to-noise approach may produce unstable results under those conditions, especially when the patient size is small. Two distributional shape parameters (alpha and beta) were estimated from the observed quality scores, and reliability was then calculated as a function of alpha, beta, and total patient count for each unit of analysis. Overall reliability in this context represents the ability of the proposed measure to confidently distinguish the performance of one entity (e.g., site) from another. A detailed description of this method is demonstrated in Section 4.2.3a. Appendix A, where we lay out the formulation of the method and describe how it improves upon the Beta-binomial approach applied in previous studies (4-8). It is commonly advised that reliability should be > 0.9 for making high-stakes decisions,
and > 0.7 for general reporting/monitoring (Eijkenaar, 2013; Adams, 2010).
REFERENCES
1. Adams, J. L., Mehrotra, A., Thomas, J. W., & McGlynn, E. A. (2010). Physician cost profiling--reliability and risk of misclassification. The New England journal of medicine, 362(11), 1014–1021. https://doi.org/10.1056/NEJMsa0906323
2. Scholle, S. H., Roski, J., Adams, J. L., Dunn, D. L., Kerr, E. A., Dugan, D. P., & Jensen, R. E. (2008). Benchmarking physician performance: reliability of individual and composite measures. The American journal of managed care, 14(12), 833–838.
3. Fung, V., Schmittdiel, J. A., Fireman, B., Meer, A., Thomas, S., Smider, N., Hsu, J., & Selby, J. V. (2010). Meaningful variation in performance: a systematic literature review. Medical care, 48(2), 140–148. https://doi.org/10.1097/MLR.0b013e3181bd4dc3
4. Adams, John L. (2009) The Reliability of Provider Profiling: A Tutorial. Santa Monica, CA: RAND Corporation. https://www.rand.org/pubs/technical_reports/TR653.html.
5. Adams, J. L., & Paddock, S. M. (2017). Misclassification Risk of Tier-Based Physician Quality Performance Systems. Health services research, 52(4), 1277–1296. https://doi.org/10.1111/1475-6773.12561
6. Blair, R., Liu, J., Rosenau, M., Brannan, M., Hazelwood, N., Gray, K. F. & Schmitt, A. (2015). Development of Quality Measures for Inpatient Psychiatric Facilities. Development, 2, 04.
7. Kazis, L. E., Rogers, W. H., Rothendler, J., Qian, S., Selim, A., Edelen, M. O.& Butcher, E. (2017). Outcome performance measure development for persons with multiple chronic conditions. RAND.
8. Staggs, V. S., & Cramer, E. (2016). Reliability of Pressure Ulcer Rates: How Precisely Can We Differentiate Among Hospital Units, and Does the Standard Signal-Noise Reliability Measure Reflect This Precision?. Research in nursing & health, 39(4), 298–305. https://doi.org/10.1002/nur.21727
9. Eijkenaar, F., & van Vliet, R. C. (2013). Profiling individual physicians using administrative data from a single insurer: variance components, reliability, and implications for performance improvement efforts. Medical care, 51(8), 731–739. https://doi.org/10.1097/MLR.0b013e3182992bc1
Reliability analyses were conducted at two levels (facility and clinician group/practice), stratified by three age categories (15-20, 21-44, and 15-44 years). More detailed information including reliability estimates for each unit at each level can be found in Section 4.2.3a. Tables 5-9.
At the facility level, reliability ranges from 0.998 to 1 for HCCN 1 and 0.976 to 0.996 for HealthEfficient for the 15-44 years age group. At the clinician group/practice level, reliability ranges from 0.998 to 1 for HCCN 1 and 0.800 to 0.999 for HealthEfficient for the 15-44 years age group. We have a small number of entities (range: 3-17) at these levels for these data partners.
See Section 4.2.3a Tables 10-13 for reliability tables by decile.
Our tested reliability is consistently greater than .90 at the facility and clinician group/practice levels for the 15-44 years age group, showing high reliability at these levels. While some entities had low overall rates on the measure, the sufficient number of patients within these entities still results in high reliability.
Overall, testing results showed that the Contraceptive Care Screening eCQM, as currently specified, can distinguish the true Contraceptive Care Screening performance in health centers and sites from one entity to another.
Validity
For HCCN 1, a total of 150 female patients aged 15-44 years in 2023 were randomly sampled from 8 sites. For HealthEfficient, a total of 144 female patients aged 15-44 years in 2023 were randomly sampled from 5 sites. For each of these patients, data elements used for the Contraceptive Care Screening measure calculation were compared between the EHR records and the patient charts, and agreement numbers were summarized in a 2 by 2 table (yes/yes, yes/no, no/yes, and no/no) for each element. We compared all 8 data elements that are required to calculate the Contraceptive Care Screening measure: had a SINC response, female sterilization, infecundity, had a qualifying encounter, had a prenatal care, had a live birth delivery date, had an estimated delivery date, and had a non-live birth. Using the patient chart as the authoritative source, we calculated sensitivity, specificity, positive predictive value (PPV), and negative predictive value (NPV) for each data element.
Results of the data element level validity analyses are shown in Section 4.3.4a Tables 1-2. We calculated sensitivity, specificity, PPV, and NPV for each data element.
Among both HCCNs, sensitivity was at least 0.7 for the majority of the data elements, whereas specificity, PPV, and NPV were above 0.7 for all data elements.
For both HCCNs, we found that the patient charts captured a small number of sterilization cases (5 in HCCN 1 and 3 in HealthEfficient), whereas standardized medical codes for sterilization were not found in the EHR data extract. This is largely because the CHCs from where the data was extracted are outpatient centers and do not provide sterilization procedure themselves. When documenting sterilization that has occurred in other sites, this can be documented in the surgical history section of their EHR systems using unstructured fields (as opposed to using ICD-10 codes to document this in the problem list).
For HCCN 1, we also found 3 live birth dates, 3 estimated delivery dates, and 1 non-live birth that were observed in the patient charts but not in the EHR data extract. This is due to the same reason as sterilization in that pregnancy outcome information was often entered into the system as history records, instead of standardized medical terminologies such as CPT or ICD codes. This level of discrepancy for these elements is expected in outpatient settings.
Overall, our data provide fairly strong evidence for validity of the Contraceptive Care Screening measure at the data element level.
Risk Adjustment
Use & Usability
Use
Usability
Health center agencies and networks can use the measure to assess whether eligible patients of reproductive age are being screened for contraceptive need. To enhance performance, entities must enact workflows that standardize annual Self-Identified Need for Contraception (SINC) screening, including patient identification, defining when, how, and by whom the patient will be asked SINC, and electronic health record (EHR) documentation.
We tested usability in pilot application of this measure in community health centers (CHCs) across the U.S. Common barriers to improvement included staff and clinician turnover, suboptimal integration into the EHR and to clinical workflows and provider resistance to SINC usage based on lack of training or comfort with contraceptive counseling or competing priorities. Despite these barriers, as documented in Section 2.4, participating CHCs were able to improve their scores through the use of quality improvement strategies, including one CHC that reached 82.1% for their Contraceptive Care Screening eCQM measure score. Another participating clinician group/practice site that achieved a screening percentage score of 98.9%. These findings indicate that this measure is responsive to change.
To enhance performance on this measure, entities would prioritize comprehensive clinician and staff training both on the importance of routine contraceptive care, contraceptive counseling skills as appropriate, and on integration of the screening tool itself, proactive leadership involvement, and the structured onboarding of new medical residents and nonclinical staff. It is also crucial to develop clear and standard workflows adapted to optimize SINC screening in the health care setting, including how to identify eligible patients for routine screening, identifying at which point and by whom SINC will be asked, working with EHR vendor to optimize SINC location in the health record.
Comments
Staff Preliminary Assessment
4655e
Importance
Strengths:
- Logic Model: A clear logic model is provided, depicting the relationships between inputs (e.g., integrating SINC into EHR workflows), activities (e.g., documenting SINC responses in the EHR), and desired outcomes (e.g., increased rates of contraceptive counseling). This model demonstrates how the measure's implementation will lead to the anticipated outcomes.
- Literature Review: The measure is supported by a comprehensive literature review that demonstrates the need for routine contraceptive screening and the reasons why the SINC question offers an advantage over existing screening questions based on pregnancy prevention frameworks.
Performance Gap: Data from pilot testing in nine Community Health Centers (CHCs) within two health care-controlled networks (HCCNs) show a performance gap. While the measure developer did not share scores by decile, they demonstrated there is substantial variation across pilot testing sites with scores ranging from 0.1% to 82.1% in one HCCN. - Existing Measures: The proposed measure addresses a healthcare need not sufficiently covered by existing measures, offering advantages in terms of patient centeredness and addressing disparities.
Patient Meaningfulness: The developer posits that the SINC screening tool was developed as a patient-centered, service-bound approach, incorporating feedback from Reproductive Justice leaders, patient advisors, and community groups to ensure it respects patient autonomy and preferences in reproductive health inquiries, allowing options like opting out to enhance comfort and relevance in clinical settings.
Limitations:
- None.
Rationale:
- The measure includes a robust evidence base, documented performance gap, significant anticipated impact, well-articulated logic model, and a rationale of its superiority over existing measures, making it essential for addressing patient needs for contraceptive access.
Closing Care Gaps
Strengths:
- The measure developer provides numerous references to scientific studies showing inequities in the provision of contraceptive care and suggests universal screening for need for contraceptive care would support efforts to address these inequities. However, they do not provide empirical data demonstrating differences in measure rates across different patient groups.
Limitations:
- However, this content alone does not address the equity criterion. The developer should consider empirically testing for differences in performance scores across multiple sociocontextual variables (e.g., race, ethnicity, urbanicity/rurality, socioeconomic status (SES), gender, gender identity, sexual orientation, age).
Rationale:
- Though the developer provided some information on inequities, no empirical testing was completed for this optional domain.
Feasibility Assessment
Strengths:
- Feasibility Assessment (Initial Endorsement): A comprehensive feasibility assessment has been conducted, demonstrating that all necessary people, tools, tasks, and technologies have been considered for the implementation of this measure. This includes a detailed analysis of the resources required and the operational steps needed to integrate the measure into current healthcare practices.
- A completed eCQM Feasibility Scorecard is attached, showing the measure was tested in at least two EHRs. All data required for this measure are readily available in a structured format, residing in fixed fields within the EHR systems tested. The data elements are accurate and coded using nationally accepted terminology standards, facilitating interoperability and standardization across different systems. Lastly, the data are captured during the course of care, ensuring that the measure does not require additional steps or disrupt normal clinical workflows.
- Adjustments Based on Feasibility: The feasibility assessment informed the final measure design, indicating decisions made to adjust the measure in response to data availability and other practical considerations.
Data Collection Strategy: Near-term paths are specified to support routine and electronic data capture with an implementable data collection strategy. Required data are routinely generated and used during care, are available in EHRs, and the data collection strategy can be implemented effectively. - Licensing and Fees: Any fees, licensing, or other requirements to use any aspect of the measure (e.g., value/code set, risk model, programming code, algorithm) are clearly described and justified.
Limitations:
- None.
Rationale:
- This new measure meets all criteria for 'Met' due to its well-documented feasibility assessment, clear and implementable data collection strategy, and transparent handling of licensing and fees, ensuring practical implementation within the healthcare system. The eCQM Feasibility Scorecard results indicate that the measure is well-supported by the current capabilities of the tested EHR systems in terms of data availability, accuracy, adherence to standards, and workflow integration. These factors collectively ensure that the measure can be implemented effectively and sustainably in a real-world healthcare setting.
Scientific Acceptability
Strengths:
- Data Sources and Dates: Data used for testing were sourced from EHRs during the calendar year 2023. Developer states that all value sets utilized in the measure rely on standardized coding systems and are published on VSAC (Value Set Authority Center). EHR data from two networks were used for reliability testing. The first network contained outpatient sites (clinician groups/practices) nested in Community Health Centers (facilities) located in Washington, Ohio, California, and Oregon. The second network contained outpatient sites nested in Community Health Centers located in Connecticut, New York, and New Jersey.
- Accountable Entity Level Reliability: The developer conducted signal-to-noise reliability testing at the accountable entity-level, which was clinician group/practice and facility level for two networks. 100% of entities at the clinician and facility levels for both networks had reliability >0.60. The developer used the empirical Bayes method to estimate signal-to-noise reliability to mitigate a small sample size for some clinician groups/practices.
Limitations:
- Data Sources and Dates: A total of nine Community Health Centers between the two networks were used for reliability testing.
Rationale:
- As a new measure, results show sufficient reliability at the clinician group/practice and facility levels using data from nine Community Health Centers across two networks. For maintenance endorsement, further data collection is needed to create a more comprehensive and representative dataset with additional accountable entities.
Strengths:
- Among both HCCNs, sensitivity was at least 0.7 for the majority of the data elements, whereas specificity, PPV, and NPV were above 0.7 for all data elements.
Limitations:
- For HCCN 1, sensitivity was below 0.7 for had a live birth delivery date, had an estimated delivery date, and had a non-live birth. The explanation was that this information (for a small number of cases) was not entered using coded data. For both HCCNs, sensitivity was below 0.7 for female sterilization. The explanation was that the sites do not perform this procedure, and documentation for the procedure performed at other sites was in unstructured fields.
Rationale:
- As a new measure, patient- or encounter-level validity testing is sufficient. Future work might focus on developing tools and resources to improve the structured coding of some required data elements.
Use and Usability
Strengths:
- Planned Use: While the measure is not currently in use, the developer indicates plans to implement the measure in public reporting, payment programs, quality improvement programs, and quality improvement efforts. The specific programs are not specified in the application.
- Actions for Improvement: The developer provides a summary of how accountable entities can use the measure results to improve performance. Specifically, facilities can improve their scores on the measure by integrating the SINC screener into clinical workflows and providing training to healthcare providers and ancillary staff on how to use the measure.
Limitations:
- None.
Rationale:
- For initial endorsement, there is a clear plan for use in at least one accountability application, and the measure provides actionable information for improvement.
Committee Independent Review
Support measure endorsement…
Importance
Criteria was met
Closing Care Gaps
Empirical testing not provided
Feasibility Assessment
Criteria was met
Scientific Acceptability
Criteria was met
Criteria was met
Use and Usability
Criteria was met
Summary
Support measure endorsement. Overall the submission shows that the measure is important for quality of care.
SINC Measure
Importance
Agree with Staff Assessment
Closing Care Gaps
Agree with Staff Assessment - understanding the impact on equitable care would help further advance this measure.
Feasibility Assessment
Agree with Staff Assessment
Scientific Acceptability
Agree with Staff Assessment
Agree with Staff Assessment
Use and Usability
Agree with Staff Assessment
Summary
I agree with statements on requiring another set of documentation is difficult this day in age, no matter if it is clinicians or staff.
I would have liked to see this SINC survey tied to increase in some sort of birth control measure improving over time as a direct result of the SINC survey. Essential tie the SINC survey back to contraceptives being used for the same age groups, equitable domains and if the compliance of SINC is up we would anticipate that the rate of patients on the contraceptive will naturally follow as per the studies references. The actual outcome being impacted by the SINC survey would be impactful.
Endorsement
Importance
Agree with staff recommendations.
Closing Care Gaps
Agree with staff recommendations.
Feasibility Assessment
Agree with staff recommendations.
Scientific Acceptability
Agree with staff recommendations.
Agree with staff recommendations.
Use and Usability
Agree with staff recommendations.
Summary
I fully endorse this measure as it addresses a need and fills a void for a critical topic which we are not currently measuring.
Agree with Staff assessment
Importance
There is evidence that the measure can address disparities and produce a narrative for providers and patients to discuss reproductive health. Current health care structures does allow for this measure to be applicable in practice.
Closing Care Gaps
Not currently addressed.
Feasibility Assessment
This measure is practical for implementation and feasibility.
Scientific Acceptability
agree with staff assessment
agree with staff assessment
Use and Usability
Detailed plan outlines plan to implement measure and ongoing improvement and accountability.
Summary
Support measure.
Endorsement of SINC measure
Importance
Logid Model: A logic model clearly outlines how integrating the SINC screening tool into EHR workflows (input), and documenting SINC responses (activity), will lead to increased rates of contraceptive counseling (desired outcome).
- Literature review: A comprehensive literature review supports the need for routine contraceptive screening, highlighting the SINC question's advantages over traditional pregnancy prevention screening questions.
- Performance gap: Pilot testing in nine Community Health Centers across two healthcare-controlled networks revealed significant performance variation, with scores ranging from 0.1% to 82.1%.
- Existing Measures: The proposed measure fills a gap in existing healthcare measures by focusing on patient-centeredness and addressing disparities in contraceptive counseling.
- Patient Meaningfulness: The SINC tool was developed in consultation with Reproductive Justice leaders, patient advisors, and community groups to ensure it respects patient autonomy and preferences, including the option to opt-out, enhancing comfort and relevance in clinical settings.
- Limitations: The report mentions no limitations.
- Rationale: The measure is justified by its robust evidence base, documented performance gap, a well-articulated logic model, and its superiority over existing measures, making it crucial for meeting patient needs in contraceptive access.
Closing Care Gaps
The developer has provided a theoretical foundation regarding inequities in contraceptive care but lacks empirical data for the optional domain of equity. There is a recommendation for the developer to conduct empirical testing across various socio-contextual variables like race, ethnicity, SES, gender identity, and more to substantiate the measure's impact on addressing health disparities.
Feasibility Assessment
- Feasibility assessment: A comprehensive assessment has been carried out, confirming that all necessary resources, including people, tools, tasks, and technologies, are accounted for in the implementation of the measure. This includes a detailed analysis of the resources and operational steps required to integrate the measure into existing healthcare practices.
- cCQM Feasibility Scorecard: The measure has been successfully tested in at least two Electronic Health Record (EHR) systems. All necessary data for this measure are structured and stored in fixed fields within these EHR systems, coded using nationally accepted standards, ensuring accuracy, interoperability, and standardization.
- Adjustments based on Feasibility: The final design of the measure has been adjusted based on the feasibility assessment, taking into consideration data availability and other practicalities.
- Data Collection strategy:: There is a clear, near-term path for routine and electronic data capture, with a strategy that ensures data are routinely generated, accessible in EHRs, and can be implemented effectively without disrupting normal clinical workflows.
- Limitations: The report mentions no limitations.
- Rationale: The measure meets all criteria due to its well-documented feasibility, effective data collection strategy, and transparent handling of licensing and fees. The results from the eCQM Feasibility Scorecard demonstrate that the measure is supported by the capabilities of the EHR systems tested, confirming its potential for effective and sustainable implementation in healthcare settings.
Scientific Acceptability
Agree with Staff assessment and comments.
Agree with Staff assessment and comments.
Use and Usability
Strengths:
- Planned use: The measure is intended for future implementation in various applications such as public reporting and quality improvement efforts, although specific programs are not detailed in the application.
Limitations:
- Only 51% of FPs, 32.4% of pediatricians, and 19.8% of internal medicine physicians prescribe contraceptives. Reasons for the relatively low numbers of PCPs prescribing contraceptives include lack of training in residency, health systems’ financial choices, insurance barriers, and expectation by some physicians and many patients that birth control belongs in the OB/GYN sector. Access, patient awareness that PCPs can provide the care, expectations, and options vary by state and region.
- Chen C, Strasser J, Banawa R, Luo Q, Bodas M, Castruccio-Prince C, Das K, Pittman P. Who is providing contraception care in the United States? An observational study of the contraception workforce. Am J Obstet Gynecol. 2022 Feb;226(2):232.e1-232.e11. doi: 10.1016/j.ajog.2021.08.015. Epub 2021 Aug 18. PMID: 34418348.
- Considering barriers beyond the scope of a PCP, the recommendation to include this measure in a payment program requires careful consideration.
Rationale:
- The measure is poised for initial endorsement due to its clear usage plans in accountability settings and its provision of actionable information for improving healthcare delivery.
Summary
While I support the endorsement of the measure, I do have concerns about barriers related to access to contraceptive care. Research by Candice Chen, MD, MPH, and colleagues found that while 73.1% of obstetrician-gynecologists (OB/GYNs) and 72.6% of nurse-midwives prescribed the pill, patch, or vaginal ring; only 51% of FPs, 32.4% of pediatricians, and 19.8% of internal medicine physicians did so.
Reasons for the relatively low numbers of PCPs prescribing contraceptives include lack of training in residency, health systems’ financial choices, insurance barriers, and expectation by some physicians and many patients that birth control belongs in the OB/GYN sector. Access, patient awareness that PCPs can provide the care, expectations, and options vary by states and regions.
While screening and counseling are critical steps, considering these barriers are beyond the scope of a PCP, the recommendation to include this measure in a payment program requires careful consideration.
Support Measure Endorsement
Importance
The Contraceptive Care Screening eCQM meets the importance criteria because it addresses a high-impact, evidence-based area of need, highlights substantial performance gaps and disparities, and aligns with national priorities for improving equitable access to reproductive care.
Closing Care Gaps
The measure was developed with a racial and health equity lens, centering patient autonomy and reducing biases. By universally screening all eligible patients, it addresses disparities in contraceptive care, particularly among Black, Latinx, LGBTQIA+, and underserved populations, aligning with principles of reproductive justice. However, there was no empirical testing provided.
Feasibility Assessment
The measure has been successfully implemented in diverse EHR systems (Epic, eCW, AthenaOne), requires minimal workflow adjustments (~1 minute per screening), and includes flexible data definitions to accommodate varying system capabilities. Challenges in data availability and workflow integration were addressed through QI initiatives, demonstrating scalability and sustained use.
Scientific Acceptability
Reliability testing at the clinician group and facility levels demonstrated strong reliability using a Beta-binomial model, with scores exceeding the threshold for general reporting (>0.7). The measure effectively distinguishes performance across entities, even in diverse clinical settings.
Validity testing showed high specificity, PPV, and NPV (>0.7) across data elements. Sensitivity was ≥0.7 for most elements, with minor discrepancies due to unstructured data in outpatient settings. Results provide strong evidence for data element validity and measure accuracy.
Use and Usability
The measure has been implemented in diverse healthcare settings, with plans to supports public reporting and quality improvement efforts.
Summary
Based on the information provided, I support endorsing this measure. It addresses a critical clinical need, demonstrates feasibility, reliability, and validity across diverse healthcare settings, and shows proven responsiveness to quality improvement initiatives.
Summary comment
Importance
This is an important metric to improve the care of female patients of childbearing age and has the potential opportunity to increase their access to reproductive health care. The question has been developed with multiple stakeholder perspectives and input.
Closing Care Gaps
Data was not provided for different racial/ethnic groups
Feasibility Assessment
This metric is comprised of a single question to patients during an episode of care. It seems like it is a feasible metric to implement as demonstrated by the pilot data provided by 2 separate healthcare systems. For clinics and health care systems to implement this metric, they would have to add this question for appropriate patients as part of the visit intake which seems relatively straightforward; however given the competing priorities that all health care systems are under these days in terms of trying to meet a variety of quality and process metrics, it may just overburden the system.
If we are saying that healthcare systems should add this metric, is there another metric that they can retire?
Scientific Acceptability
High reliability based on metric provided
I think the main challenge with this metric is trying to identify the appropriate denominator given that many patients go to different places for care and the EHR data may not be accessible across these sites of care. The sensitivity for some of the codes seems low and it would be important to test this metric across a broader variety of healthcare systems.
Use and Usability
Clinics and health care systems could implement this metric as part of routine intake for patients. I think the biggest hurdle would be extracting the data from the EHR to assess performance on the metric to ensure that the denominator is accurate.
Summary
This is an important metric and will likely improve the care of female patients of childbearing age. The measure developer have submitted preliminary data suggesting that the metric can be reliably accessed and is valid. The metric has the support of many professional and advocacy organizations. The preliminary data provided can be augmented to further demonstrate feasibility in more diverse health care systems and among different racial/ethnic groups. The main concern is adding another performance metric to already burdened health care systems.
Endorsement of 4655e
Importance
This measure is important. It aims to improve rates of contraceptive counseling to patients who want it. It addresses a sizable gap in care, based on existing data cited by the developer. Additionally, it is aligned with goals of the CDC and ACOG to promote proactive pregnancy counseling.
Closing Care Gaps
Equity is not a required domain. In the future, the measure should be risk stratified to show measure rates by different patient groups.
Feasibility Assessment
The feasibility of the eCQM was tested and implemented in two different electronic health records (EHR) systems: HCCN 1 utilizes its customized version of Epic, and HealthEfficient uses eClinicalWorks (eCW).
The developer notes that EHR changes took about three months in collaboration with clinical and vendor teams.
HealthEfficient indicated that 15% of the eCQM data elements scored 0 in the Data Availability feasibility domain (i.e., data are readily available in a structured format), 20% scored 0 in the Data Accuracy domain (i.e., information contained in the data is correct), 30% scored 0 in the Data Standards domain (i.e., data element is coded using a nationally accepted terminology standard and mapped to the QDM), and 38% scored 0 in the Workflow domain (i.e., extent to which data element capture impacts the workflow for the user).
HCCN 1 reported that 5-10% of eCQM data elements scored 0 for availability, accuracy, and standards, while 13% scored 0 for workflow..
Given the feasibility issues identified during testing and lack of data standardization, the developer needs to provide a clearer and less burdensome plan for integration of the SINC data element into EHRs.
Scientific Acceptability
Reliability analyses were conducted at two levels (facility and clinician group/practice) and demonstrated high reliability with results greater than .9
While data element validity scores were high, there were some discrepancies identified. This was largely due to the data elements not being standardized, including the following specific items:
- Sterilization: the developer states that this can be documented in the surgical history section of their EHR systems using unstructured fields. However, unstructured data are threats to validity given the inconsistency of free text documentation
- Live birth dates
- Estimated delivery dates
- Non-live births
Use and Usability
Despite described barriers to improvement including clinician resistance to use the SINC due to lack of training or comfort with contraceptive counseling, the developer provides data demonstrating that CHCs were able to improve their scores through the use of quality improvement strategies.
Summary
Overall, I support the endorsement of 4655e. My major concern is the feasibility of this measure and the burden of integrating SINC into EHRs.
SINC eCQM Endorsement
Importance
This measure addresses an important gap in care relevant to a large population of patients.
Closing Care Gaps
Agree with staff assessment and other commenters. Measure developers established potential gains in health equity by improvements in this measure. However, there was not data demonstrating disparities across patient groups on the SINC question. Implementing this measure could help to provide data in this area and allow for this to be addressed more thoroughly in measure maintenance.
Feasibility Assessment
Implementation of this eCQM is feasible and straightforward. The numerator evaluates completion of a single question, and the other measure criteria rely on data elements already in use for other measures and readily available.
Scientific Acceptability
Agree with staff assessment
Agree with staff assessment
Use and Usability
Agree with staff assessment
Summary
Agree with the staff assessment on all domains
Public Comments
Support for Contraceptive Care Screening eCQM (CBE ID: 4655e)
Going to: Partnership to Quality Measure (PQM) by Battelle. PQM is a consensus-based CMS certified entity that uses a consensus-based process involving a variety of experts - clinicians, patients, measure experts, and health information technology specialists - to ensure informed and thoughtful endorsement reviews of qualified measures. PQM has opened a measure Contraceptive Care Screening eCQM (CBE ID: 4655e) for public comment until 11:59pm ET December 16, 2024.
Context: We have been asked by USCF to submit a comment in support of SINC inclusion in eCQM, since in the past we have been supportive of SINC. The electronic Clinical Quality Measure (or eCQM), utilizes the Self-Identified Need for Contraception (SINC) screening question to assess whether individuals are being asked about their contraceptive need. Since the primary partnership/contact of USCF is our department of Medical Services, and since the focus of the comment is on quality care (and PQM looks for clinicians and measure experts), we have decided that June Gupta, from Medical Services, is the best person to submit the comment.
RE: Support for Contraceptive Care Screening eCQM (CBE ID: 4655e)
Planned Parenthood Federation of America (PPFA) is pleased to submit this comment letter expressing its support for the Contraceptive Care Screening electronic Clinical Quality Measure (eCQM)’s integration of the Self-Identified Need for Contraception (SINC) released by Partnership for Quality Measures (PQM). PPFA has consistently supported University of California San Francisco (UCSF)’s Person-Centered Reproductive Health Program SINC measurement. We are aware UCSF has engaged in extensive stakeholder engagement to develop this measure, including through collaboration with Coalition to Expand Contraceptive, the National Family Planning & Reproductive Health Association Access and reproductive justice consultants. These efforts sought to ensure that the SINC question is patient-centered and avoids the potential to be perceived as judging or targeting individuals’ reproductive choices. As a trusted advocate for sexual and reproductive health (SRH) and national representative of Planned Parenthood health centers, PPFA appreciates the opportunity to weigh in on policy proposals that impact the communities we serve across the country –like is the case with this proposal by PQM. PPFA is also deeply concerned about issues impacting people’s privacy, such as interoperability.
PPFA is a 501(c)(3) charitable organization that supports the independently incorporated Planned Parenthood affiliate health centers across the United States. Planned Parenthood health centers are the nation’s most trusted, nonprofit source of primary and preventive care for people of all genders, and they are also the nation’s largest sex educator and provider of information on healthy relationships. PPFA and its affiliated health center providers are experts on meeting people where they are through innovative apps, chat programs, and culturally responsive care for young people, LGBTQ+ patients, and patients of color.
Each year, Planned Parenthood health centers provide affordable birth control, lifesaving cancer screenings, testing and treatment for sexually transmitted infections (STIs), abortion, and other essential care to 2.1 million patients annually, and ensure that all people have accurate information about sexual and reproductive health. Notably, one in three women in the United States has visited a Planned Parenthood health center. The majority (nearly 70%) of Planned Parenthood patients have incomes at or below 150 percent of the Federal Poverty Level (FPL).
Planned Parenthood health centers provide health care, education and information for lesbian, gay, bisexual, transgender, queer and gender-nonconforming people, women, communities of color, immigrants, people with chronic illnesses and disabilities, and others who frequently experience systemic oppression and barriers to care. Therefore, PPFA and our health centers are acutely aware of the racism, homophobia, xenophobia, transphobia, and sexism that is rooted in our society, and how these systems of oppression impact people’s health. Incentivizing patient-centered contraceptive care screening through use of an eCQM can enable tracking of quality contraceptive access within a safety net system and facilitate ongoing quality improvement, supporting reproductive health equity.
Thus, PPFA is providing feedback to the Contraceptive Care Screening eCQM’s integration of the SINC released by Partnership for Quality Measures because we recognize performance measures provide a critical tool for promoting patient-centered contraceptive access in the United States, which is particularly important in the current environment in which reproductive autonomy is increasingly being threatened. Additionally, we are commenting to express our concerns and the need for a balance between equitable collection of contraceptive health information and protecting individual patients’ privacy.
The development of an eCQM for contraceptive care screening aligns contraceptive quality measurement with the next generation of performance measurement. Thus, we support the integration of the SINC into clinic workflows since it is a critical step towards centering people’s needs as they themselves define them in the context of contraceptive quality measurement. However, PPFA is also aware that electronic collection, storage and sharing of the health information related to a patient’s sexual and reproductive health care, such as contraceptive information, could lead to substantial harm, including criminalization.
Generally, PPFA supports expanding health data collection and exchanges for the benefit of patients, its communities, and for public health. However, we are always careful in considering interoperability and electronic data collection expansions, since the current hostile political and legal landscape for reproductive care represents a data privacy risk to our patients’ safety, as well as the safety of their families and providers. While expanding access for contraception is critical, it is not a solution to the abortion access crisis, as contraception cannot fully address the need for safe and legal abortions.
For context, the Dobbs v. Jackson Women’s Health Organization U.S. Supreme Court decision led to numerous states prohibiting or severely restricting access to abortion. The abortion bans that have been enacted have caused access to contraceptive care to become increasingly threatened. The consequences of criminalizing sexual and reproductive health care can include investigations, arrests, civil penalties, loss of children, and reputational harm. In particular, individuals' access to contraceptive options like intrauterine devices (IUDs) and emergency contraceptive pills are often mistakenly alleged to cause abortions. This misconception, along with the definitions utilized in abortion bans enacted by certain states, could potentially serve as means to restrict access to contraception. For example, definitions in abortion bans that establish the existence of a pregnancy from the moment of fertilization could be construed to mean that preventing the implantation of a fertilized egg equals terminating a pregnancy – therefore potentially banning certain types of contraception.
While interoperability facilitates record sharing for patient-centered care, it also increases opportunities for utilizing a patient’s pregnancy data against them, including a patient’s contraceptive data. Since the Contraceptive Care Screening and its integration of SINC collects data of the type of contraception a patient currently has or wants, the out-of-state sharing of contraceptive health information to an abortion-restricted state could potentially cause a patient or a provider to unjustly suffer criminalization for seeking or providing essential health care where it was lawful to do so. To mitigate this harm, PQM should make sure that the patient has the ability to request a restriction on sharing their Contraceptive Care Screening data, including SINC.
PPFA is grateful for the opportunity to share its perspective on Contraceptive Care Screening eCQM’s integration of the SINC released by Partnership for Quality Measures, as a provider of sensitive health care services. We are available to support this initiative as needed as PQM moves toward finalizing this and other electronic clinical system innovations. Please do not hesitate to reach out to me at [email protected] for additional information.
Respectfully,
June Gupta, NP
National Director, Medical Services
Planned Parenthood Federation of America
1110 Vermont Avenue NW, Suite 300
Washington, DC 20005
Hello June and PPFA team! We…
Hello June and PPFA team! We thank you for submitting your comment and for your support for SINC as a person-centered screening tool. We want to echo your concerns about patient safety and data security, especially in our ever-changing policy landscape. We agree confidentiality is central to health care delivery and SINC data should be protected in alignment with all other types of reproductive health data. Patients should be able to request restrictions on their data, as their safety is our paramount priority. We believe there are clear steps healthcare systems can take to proactively protect their patients and will incorporate this strong recommendation in implementation guidance for the measure.
Support for Contraceptive Care Screening eCQM
The National Family Planning & Reproductive Health Association (NFPRHA) is pleased to express its strong support for the University of California, San Francisco (UCSF) Person-Centered Reproductive Health Program’s application for the Contraceptive Care Screening Electronic Clinical Quality Measure (eCQM) (CBE ID: 4655e).
As a non-partisan, nonprofit membership association whose mission is to advance and elevate the importance of family planning in the nation’s health care system and promote and support the work of family planning providers and administrators, especially in the safety net, NFPRHA is well-positioned to provide feedback on the new Contraceptive Care Screening eCQM. NFPRHA’s membership includes nearly 1,000 entities that operate or fund more than 3,500 health centers that deliver high-quality family planning and sexual health services to millions of people in the US every year. Comprised of 67 of the 86 grantee organizations currently funded by the Office of Population Affairs (OPA) through the Title X Family Planning Program, NFPRHA’s organizational members include state, county, and local health departments; private, nonprofit family planning organizations; family planning councils; Planned Parenthood affiliates, hospital-based clinics; and federally qualified health centers.
Providing individuals who do not desire to become pregnant with access to contraceptive services is an essential component of a quality health care system that optimizes reproductive health and wellness. The Contraceptive Care Screening eCQM complements existing performance measures related to contraceptive care by adding a dimension to the quality care pathway: screening for contraceptive need. Improving contraceptive care delivery in the US is especially important given that the provision of such services has a history partially rooted in reproductive coercion and a fundamental devaluing of the bodily autonomy of people of color and those with no or low incomes. Asking about contraception and pregnancy prevention in health care setting carries the weight of this history. Therefore, NFPRHA believes it is critical that screening for contraceptive need is done in a manner that does not inadvertently reproduce harm by communicating a sense of expectation or pressure to use contraception.
Developed by the Person-Centered Reproductive Health Program at UCSF in consultation with race equity and Reproductive Justice leaders, the Self-Identified Need for Contraception (SINC) question assesses whether the patient would like contraceptive care services as part of that day’s visit. By prioritizing that each patient receives the services they want and need as part of their visit, the Contraceptive Care Screening eCQM—which measures the percentage of patients assigned female at birth and aged 15-44 years who were asked the SINC question with a recorded response—represents a welcomed shift away from the traditional, potentially harmful approach of assessing patients’ service needs using a triangulated approach of categorizing them as “at risk” of unintended pregnancy based on factors that may or may not be relevant.
NFPRHA looks forward to collaborating with UCSF and its partners to promote the uptake and widespread use of the Contraceptive Care Screening eCQM in family planning and sexual health settings and beyond.
Sincerely,
Clare Coleman
President & CEO
National Family Planning & Reproductive Health Association
Thank you so much, Clare and…
Thank you so much, Clare and the NFPRHA team! We greatly appreciate your support in this work and look forward to our continued partnership to further promote access to equity-based, person-centered contraceptive care.
Endorsement for the Contraceptive Care Screening eCQM
Dear Colleagues at the Partnership for Quality Measurement (PQM),
Thank you for the opportunity to comment on the Contraceptive Care Screening eCQM (CBE ID: 4655e). We at the Coalition to Expand Contraceptive Access (CECA) are writing to strongly urge you to endorse the Contraceptive Care Screening eCQM.
CECA is a convener of committed partners working to ensure access to contraception as part of a broader vision to achieve sexual and reproductive health equity (SRHE) for the US. Through evidence reviews and extensive collaboration, CECA works to advance quality measurement by clarifying the value of contraceptive care measures, highlighting their potential, and prioritizing opportunities.
Sexual and reproductive health is an integral part of people’s health and wellbeing, and people value access to high-quality sexual and reproductive health care that respects their needs, goals, preferences, and choices. To improve the health care system’s ability to center and meet the needs of all people – and minimize the risk of coercion and stigma in sexual and reproductive health care – we sorely need values-aligned measures that drive quality improvement and culture shift in clinical practice and policy. Importantly, we must prioritize measures that are developed with principles of person-centeredness, reproductive justice, and SRHE at their core, such as the Contraceptive Care Screening eCQM.
Few performance measures currently exist for contraceptive care. Diverse audiences, including providers, federal and state policymakers, evaluators/researchers, private sector partners, community-based organizations, advocates, and patients have expressed how essential it is to enhance contraceptive care measurement and, ultimately, the role that comprehensive, valid, and reliable measurement plays in advancing sexual and reproductive health and wellbeing broadly. Implementing the Self-Identified Need for Contraception (SINC) screening question is a needed step in this direction because it helps drive providers to prioritize individuals’ needs and, more so, gives individuals more autonomy over their clinical encounter and health. Measures that result from implementing SINC, including the Contraceptive Care Screening eCQM, generate insights on where/how health centers can further prioritize and improve person-centered practice. Further, assessing the Contraceptive Care Screening eCQM across different communities of people builds our ability to understand and address inequities in care. Used in tandem with the Person-Centered Contraceptive Counseling (PCCC) measure and the Contraceptive Use eCQMs, the Contraceptive Care Screening eCQM contributes to a more holistic understanding of contraceptive access and equity across the different stages of care. In primary care settings, this advancement in measurement can drive prioritizing and integrating sexual and reproductive care into routine, essential health care, in a person-centered way.
An endorsement of the Contraceptive Care Screening eCQM from PQM will align with and strengthen the adoption and promotion of SINC across federal agencies, health systems, and the field. As mentioned, your endorsement of this measure can also improve the provision and quality of person-centered contraceptive care, and advance strategies to make contraceptive access more equitable. Now is a crucial time to move comprehensive contraceptive care quality measures forward when sexual and reproductive health is becoming increasingly threatened.
Thank you for your thoughtful consideration. Please feel free to contact us at [email protected] if you have any questions.
Warmly,
The Coalition to Expand Contraceptive Access
https://www.contraceptionaccess.org/
Thank you CECA team for your…
Thank you CECA team for your wonderful comment! We appreciate your partnership in the advancement of equitable, person-centered measures, with the ultimate goal of sexual and reproductive health equity (SRHE) for all people.
SINC Measure Public Comment
On behalf of the American College of Obstetricians and Gynecologists (ACOG), representing more than 62,000 physicians and partners dedicated to advancing women’s health and the health of individuals seeking obstetric and gynecologic care, we greatly appreciate the opportunity to provide feedback on the new Contraceptive Care Screening eCQM.
The benefits of contraception, named as one of the 10 great public health achievements of the 20th century by the Centers for Disease Control and Prevention, are widely recognized and include improved health and well-being, reduced global maternal mortality, health benefits of pregnancy spacing for maternal and child health, female engagement in the work force, and economic self-sufficiency for women. ACOG supports access to comprehensive contraceptive care and methods as an integral component of women’s health care. We are also committed to encouraging and upholding policies and actions that ensure the availability of affordable and accessible contraceptive care and methods. Furthermore, ACOG advocates for continual improvements in the quality of care provided to our member’s patients and smooth transitions for our members to better engage in the space of quality improvement.
While contraceptive care access measures exist in the United States, a focus on self-identified need for contraception has been lacking. Endorsing such a measure as the new Contraceptive Care Screening eCQM will help fill the void with respect to adequate provision of and counseling around contraception. This measure will enhance our current repertoire of contraception-focused measures and enhance the patient-centeredness of contraceptive care across the country. As such, ACOG recommends endorsing the Contraceptive Care Screening eCQM as written.
Hello ACOG team! Thank you…
Hello ACOG team! Thank you so much for your comment, we deeply appreciate your support of this measure.
Supporting CBE #4655e - Contraceptive Care Screening eCQM
The Primary Care Development Corporation appreciates the opportunity to comment on CBE #4655e - Contraceptive Care Screening eCQM.
High quality, integrated, patient-centered primary care saves lives, leads to better individual and community health, and is central to health equity. Primary care is the foundation of our health care system and is key to preventing treatable outpatient diseases – like diabetes and heart disease – from turning into life threatening conditions. Further, primary care encompasses a wide range of sexual and reproductive health care, including contraceptive care. Women[i] see their primary care providers substantially more than men[ii], especially during their reproductive years, and reproductive health care services, including those provided in primary care settings, are essential for the 72 million women of reproductive age in the US.[iii] Patient-centered medical care, particularly for women and others who can become pregnant and are of reproductive age, should include an assessment of contraception need. There are a number of models for identifying patient contraception need and intention, but this particular proposal, the Self Identified Need for Contraception, was developed by the UCSF’s Person-Centered Reproductive Health Program, with extensive stakeholder engagement, including through collaboration with reproductive justice consultants, the Coalition to Expand Contraceptive Access, and the National Family Planning and Reproductive Health Association. These efforts sought to ensure that the SINC question is patient-centered and avoids the potential to be perceived as judging or targeting individuals’ reproductive choices. As a result, using this question is more likely to identify actual patient need while building trust with patients.
Uptake of the Contraceptive Care Screening eCQM can incentivize person-centered integration of contraceptive care provision in primary care – meeting the needs and preferences of many patients – including in Federally Qualified Health Centers (FQHCs).
In particular, there is increasing attention to the importance of contraceptive care provided in FQHCs, which provide care to many individuals who experience barriers accessing contraception and are more likely to be used by women who are low-income, women of color, and publicly insured or uninsured. Incentivizing patient-centered contraceptive care screening through use of this measure can enable tracking of quality contraceptive access within this safety net system and facilitate ongoing quality improvement, supporting reproductive health equity.
It is important to note, however, that primary care providers already suffer from enormous administrative burdens, which keep them from their patients, add hours of additional work to their day, and ultimately contribute to burn-out and loss of providers from the field.[iv] Despite the overwhelming evidence supporting the population health benefits of more primary care providers, the per capita supply of primary care physicians has decreased over recent decades.[v] Part of the reason for this decrease in provider supply is this overwhelming administrative burden.[vi] Because primary care has been proven to be effective in achieving better outcomes at lower costs, primary care providers continually face new demands, including new screenings and integration of new models and types of care. Research has shown that primary care appointments are often more complicated than other types of medical appointments, both in terms of the number of conditions and medications to address and the number of codes to bill as a result.[vii] Further, recent research indicates that primary care providers who participate in value based payment systems are responsible for meeting an average of 57 quality measures, an intense burden on already overwhelmed practices.[viii] While PCDC supports the inclusion of contraceptive care and screening into primary care and believe that this measure is important, we also believe that it is important to minimize the number of requirements on primary care providers to ensure that we do not further exacerbate burn out and loss from the field.
[i] In addition to women, other individuals who do not identify as women, including transgender men and some non-binary people, may also have the capacity to become pregnant and need access to comprehensive reproductive health care, including contraception.
[ii] Centers for Disease Control and Prevention, National Center for Health Statistics, Press Release, New Study Profiles Women’s Use of Health Care: Women more likely than men to visit the doctor, more likely to have annual exams, July 26, 2001, available at https://www.cdc.gov/nchs/pressroom/01news/newstudy.htm.
[iii] Guttmacher Institute, Fact Sheet, Contraception Use in the United States, May 2021, available at https://www.guttmacher.org/fact-sheet/contraceptive-use-united-states.
[iv] Shari M. Erikson et al. , Putting Patients First by Reducing Administrative Tasks in Health Care: A Position Paper of the American College of Physicians, Annals of Internal Medicine, Position Paper, May 2, 2017, available at https://www.acpjournals.org/doi/10.7326/m16-2697 .
[v] Sanjay Basu et al., Estimated Effect on Life Expectancy of Alleviating Primary Care Shortages in the United States, Annals of Internal Medicine July 2021, available at https://www.acpjournals.org/doi/10.7326/M20-7381.
[vi] Shari M. Erikson et al., Putting Patients First by Reducing Administrative Tasks in Health Care: A Position Paper of the American College of Physicians, Annals of Internal Medicine, Position Paper, May 2, 2017, available at https://www.acpjournals.org/doi/10.7326/m16-2697 .
[vii] Id.; see also Joshua Freeman, Stephen Petterson, & Andrew Bazemore, Accounting for Complexity: Aligning Current Payment Models with the Breadth of Care by Different Specialties, American Family Physician Graham Center Policy One Pager, 2014, available at https://www.aafp.org/pubs/afp/issues/2014/1201/p790.pdf.
[viii] Claire Boone, Anna Zink, Bill J. Wright, Value-Based Contracting in Clinical Care, JAMA Health Forum, Research Letter, Aug. 23, 2024, https://jamanetwork.com/journals/jama-health-forum/fullarticle/2822685 (last visited Sept. 2, 2024).
Hello Primary Care…
Hello Primary Care Development Corporation team! Thank you so much for this comment. We appreciate and agree that there is a real need to attend to data burden and issues of burnout in the healthcare workforce. SINC is designed to be collected as part of routine care delivery and patient-centered clinical workflows. We paid special attention to ensuring the burden of data collection and reporting is minimized.
Endorsement for the Contraceptive Care Screening eCQM
Dear Colleagues at the Partnership for Quality Measurement (PQM),
Thank you for the opportunity to comment on the Contraceptive Care Screening eCQM (CBE ID: 4655e). We at the Coalition to Expand Contraceptive Access (CECA) are writing to strongly urge you to endorse the Contraceptive Care Screening eCQM.
CECA is a convener of committed partners working to ensure access to contraception as part of a broader vision to achieve sexual and reproductive health equity (SRHE) for the US. Through evidence reviews and extensive collaboration, CECA works to advance quality measurement by clarifying the value of contraceptive care measures, highlighting their potential, and prioritizing opportunities.
Sexual and reproductive health is an integral part of people’s health and wellbeing, and people value access to high-quality sexual and reproductive health care that respects their needs, goals, preferences, and choices. To improve the health care system’s ability to center and meet the needs of all people – and minimize the risk of coercion and stigma in sexual and reproductive health care – we sorely need values-aligned measures that drive quality improvement and culture shift in clinical practice and policy. Importantly, we must prioritize measures that are developed with principles of person-centeredness, reproductive justice, and SRHE at their core, such as the Contraceptive Care Screening eCQM.
Few performance measures currently exist for contraceptive care. Diverse audiences, including providers, federal and state policymakers, evaluators/researchers, private sector partners, community-based organizations, advocates, and patients have expressed how essential it is to enhance contraceptive care measurement and, ultimately, the role that comprehensive, valid, and reliable measurement plays in advancing sexual and reproductive health and wellbeing broadly. Implementing the Self-Identified Need for Contraception (SINC) screening question is a needed step in this direction because it helps drive providers to prioritize individuals’ needs and, more so, gives individuals more autonomy over their clinical encounter and health. Measures that result from implementing SINC, including the Contraceptive Care Screening eCQM, generate insights on where/how health centers can further prioritize and improve person-centered practice. Further, assessing the Contraceptive Care Screening eCQM across different communities of people builds our ability to understand and address inequities in care. Used in tandem with the Person-Centered Contraceptive Counseling (PCCC) measure and the Contraceptive Use eCQMs, the Contraceptive Care Screening eCQM contributes to a more holistic understanding of contraceptive access and equity across the different stages of care. In primary care settings, this advancement in measurement can drive prioritizing and integrating sexual and reproductive care into routine, essential health care, in a person-centered way.
An endorsement of the Contraceptive Care Screening eCQM from PQM will align with and strengthen the adoption and promotion of SINC across federal agencies, health systems, and the field. As mentioned, your endorsement of this measure can also improve the provision and quality of person-centered contraceptive care, and advance strategies to make contraceptive access more equitable. Now is a crucial time to move comprehensive contraceptive care quality measures forward when sexual and reproductive health is becoming increasingly threatened.
Thank you for your thoughtful consideration. Please feel free to contact us at [email protected] if you have any questions.
Warmly,
The Coalition to Expand Contraceptive Access
https://www.contraceptionaccess.org/
Thank you CECA team for your…
Thank you CECA team for your wonderful comment! We appreciate your partnership in the advancement of equitable, person-centered measures, with the ultimate goal of sexual and reproductive health equity (SRHE) for all people.
in support of the SINC screening questions
As Medical Director of Sexual and Reproductive Health at The Cambridge Health Alliance, we decided to use the SINC as our contraception screener and screen all genders. The SINC embraces the concept of ask patients "what matters to me" in a respectful way. Patients may not feel comfortable sharing pregnancy intention and/or judged by the question from a care team member since it may occur without context. Patients are also aware that there is limited time in a visit and the SINC allows them to decide whether contraception is a topic they wish to explore that day. We have excellent screening results using this tool and we highly recommend that this become the tool of choice for contraceptive screening in the US.
Thank you Kirsten and the…
Thank you Kirsten and the Cambridge Health Alliance team for your supportive comment! It's wonderful to hear patients are responding positively to the SINC screening question.
Public Comment Shared During November 21 Listening Session
My name is Rebekah Fries. I'm a policy and advocacy manager with Upstream USA, and we appreciate the opportunity to comment on CBE #4655e - Contraceptive Care Screening eCQM.
Upstream is a nonprofit organization working to expand access to contraception by providing high quality, patient-centered training and technical assistance to health care organizations.
There are very few nationally endorsed measures that focus on contraceptive care, and we believe that including this screening-focused measure will greatly improve the ability to monitor and measure access to and provision of essential contraceptive services in the US. Since our founding in 2014, Upstream has partnered with over 130 health care organizations across 30 states to integrate high quality patient-centered contraceptive care into primary care.
A foundational component of our work is helping health care teams configure their electronic health records to support a contraceptive care workflow, which begins with a contraceptive need screening question. And an increasing number of our partners specifically choose to implement the self-identified need for contraception, also known as SINC. So, we know that this eCQM would be able to be leveraged by the field.
Upstream strongly encourages the Partnership for Quality Measurement to endorse the contraceptive care screening eCQM, and doing so would align with and support other recent efforts to broaden the use of and facilitate reporting the use of SINC. Specifically, endorsing this eCQM for contraceptive needs screening aligns with efforts of OPA, the Office of Population Affairs, to encourage Title 10 clinics to report this information through FPAR 2.0. And in addition, in April 2024, the Health Resources and Services Administration, also known as HRSA, announced contraceptive need screening as a new reporting requirement for Federally Qualified Health Centers (FQHCs) for the 2024 calendar year. Taking these two together, these two reporting changes mean that roughly 3,800 service sites funded through Title 10, as well as the more than 15,000 service sites funded through the Health Center Program, are expected to report on how often patients are screened for their desire to receive contraceptive care in a particular visit. And additionally, in an August 2024 informational bulletin, the Centers for Medicare & Medicaid Services recommended SINC as an emerging measure to be considered for broader use development and potentially included in future iterations of the Core Sets. Lastly, the Office of the National Coordinator for Health Information Technology released a maternal health data set for public comment in May 2024. This data set, which has yet to be finalized, also includes SINC.
So again, just to reiterate, Upstream strongly encourages endorsement of the contraceptive care screening eCQM and we thank you for your time and your consideration.
Thank you so much Rebekah…
Thank you so much Rebekah for attending the public comment listening session and submitting this endorsement of our measure! We greatly appreciate Upstream's continuous partnership and support of this work.
Contraceptive Care Screening eCQM (CBE ID: 4655e)
I am writing to request PQM endorsement of the contraceptive care screening measure.
I am a primary care provider in a Federally Qualified Health Center in Maryland and Medical Director of Population Health. In a few of my published works, A Mixed Methods Study of Contraceptive Counseling and Care at a Federally Qualified Health Center in Maryland, I call for improved measurement systems for contraceptive management (which begins with screening for any need for contraceptive counseling). We have implemented SINC at our clinic and it has helped move the needle toward more fully promoting reproductive autonomy of the people we serve.
Thanks so much, Chase…
Thanks so much, Chase Brexton team! We are thrilled SINC is helping improve care at your site.